
Lab 4: Skeletal System I – Bone Tissue and Axial Skeleton
Bone structures, Axial Skeleton
When you are prepared for the Test on Week 4 Learning Objectives in Week 5, you will be able to:
- Identify components of long bone structure and their functions.
- Identify components of bone tissue.
- Identify zones of the epiphyseal plate and describe how the activities in each zone contribute to bone growth.
- Identify the bones of the axial skeleton, including all of those in the skull.
- Identify some of the important morphological features of the skull, which bones they are located in, and their functions (listed in the lab activity).
- Identify the major sutures of the skull.
- Identify the major regions of the vertebral column, the rib cage, and the sternum.
The skeletal system forms the rigid internal framework of the body. It consists of the bones, cartilages, and ligaments. Bones support the weight of the body, allow for body movements, and protect internal organs. Cartilage provides flexible strength and support for body structures such as the thoracic cage, the external ear, and the trachea and larynx. At joints of the body, cartilage can also unite adjacent bones or provide cushioning between them. Ligaments are the strong connective tissue bands that hold the bones at a moveable joint together and serve to prevent excessive movements of the joint that would result in injury. Providing movement of the skeleton are the muscles of the body, which are firmly attached to the skeleton via connective tissue structures called tendons. As muscles contract, they pull on the bones to produce movements of the body. Thus, without a skeleton, you would not be able to stand, run, or even feed yourself!
The Functions of the Skeletal System
Bone, or osseous tissue, is a hard, dense connective tissue that forms most of the adult skeleton, the support structure of the body. In the areas of the skeleton where bones move (for example, the ribcage and joints), cartilage, a semi-rigid form of connective tissue, provides flexibility and smooth surfaces for movement. The skeletal system is the body system composed of bones and cartilage and performs the following critical functions for the human body:
- supports the body
- facilitates movement
- protects internal organs
- produces blood cells
- stores and releases minerals and fat
Support, Movement, and Protection
The most apparent functions of the skeletal system are the gross functions—those visible by observation. Simply by looking at a person, you can see how the bones support, facilitate movement, and protect the human body.
Just as the steel beams of a building provide a scaffold to support its weight, the bones and cartilage of your skeletal system compose the scaffold that supports the rest of your body. Without the skeletal system, you would be a limp mass of organs, muscle, and skin.
Bones also facilitate movement by serving as points of attachment for your muscles. While some bones only serve as a support for the muscles, others also transmit the forces produced when your muscles contract. From a mechanical point of view, bones act as levers and joints serve as fulcrums. Unless a muscle spans a joint and contracts, a bone is not going to move.
Bones also protect internal organs from injury by covering or surrounding them. For example, your ribs protect your lungs and heart, the bones of your vertebral column (spine) protect your spinal cord, and the bones of your cranium (skull) protect your brain.
Mineral Storage, Energy Storage, and Hematopoiesis
On a metabolic level, bone tissue performs several critical functions. For one, the bone matrix acts as a reservoir for a number of minerals important to the functioning of the body, especially calcium, and phosphorus. These minerals, incorporated into bone tissue, can be released back into the bloodstream to maintain levels needed to support physiological processes. Calcium ions, for example, are essential for muscle contractions and controlling the flow of other ions involved in the transmission of nerve impulses.
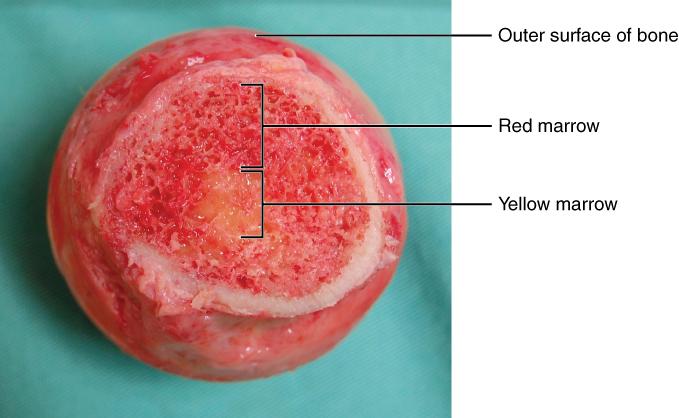
Bone also serves as a site for fat storage and blood cell production. The softer connective tissue that fills the interior of most bone is referred to as bone marrow. There are two types of bone marrow: yellow marrow and red marrow. Yellow marrow contains adipose tissue; the triglycerides stored in the adipocytes of the tissue can serve as a source of energy. Red marrow is where hematopoiesis—the production of blood cells—takes place. Red blood cells, white blood cells, and platelets are all produced in the red marrow.
Bone Classification
The 206 bones that compose the adult skeleton are divided into five categories based on their shapes (Figure 4.1). Their shapes and their functions are related such that each categorical shape of bone has a distinct function.
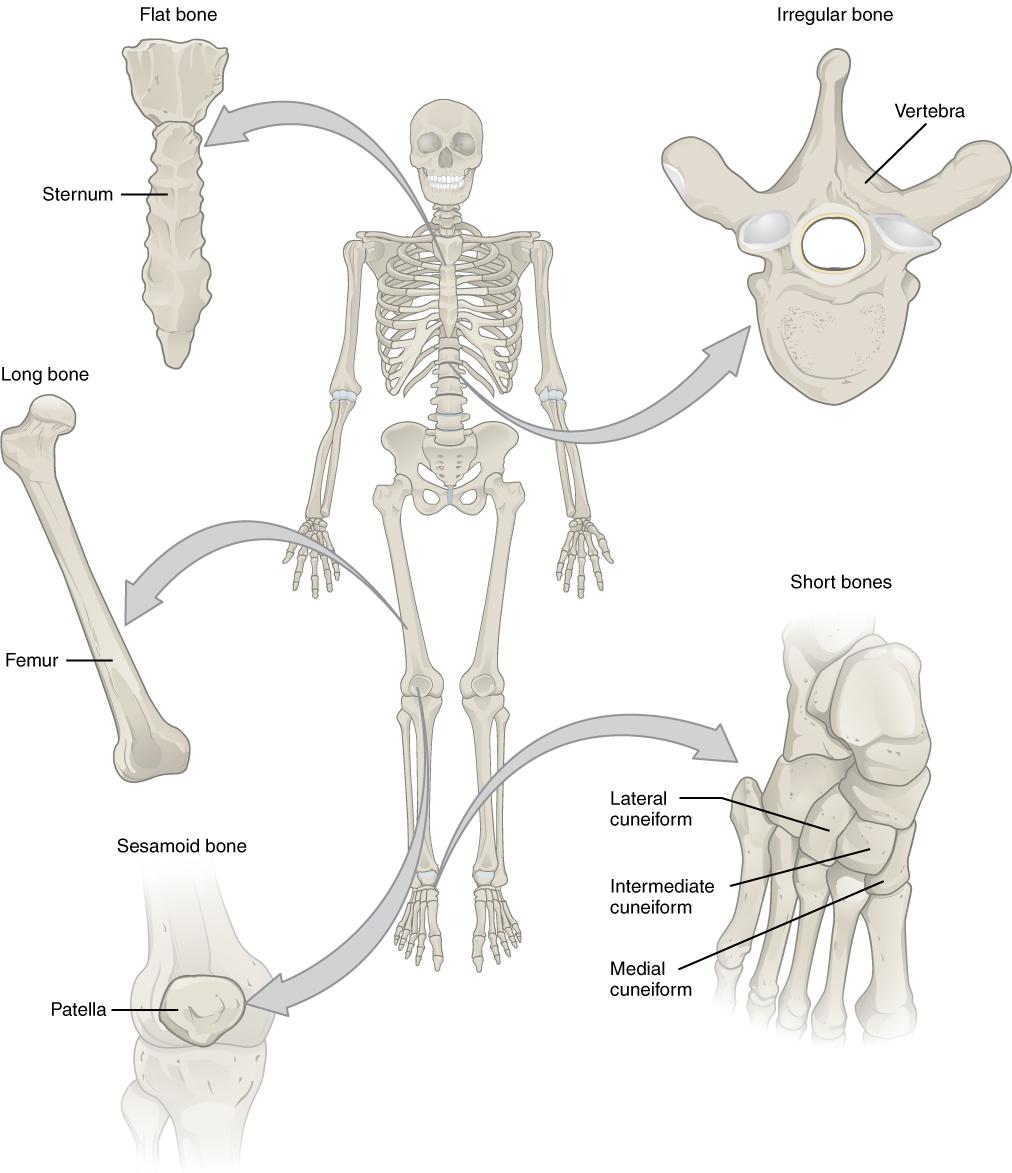
- Long Bones – A long bone is one that is cylindrical in shape, being longer than it is wide. Keep in mind, however, that the term describes the shape of a bone, not its size. Long bones are found in the arms (humerus, ulna, radius) and legs (femur, tibia, fibula), as well as in the fingers (metacarpals, phalanges) and toes (metatarsals, phalanges). Long bones function as levers; they move when muscles contract.
- Short Bones – A short bone is one that is cube-like in shape, being approximately equal in length, width, and thickness. The only short bones in the human skeleton are in the carpals of the wrists and the tarsals of the ankles. Short bones provide stability and support as well as some limited motion.
- Flat Bones – The term “flat bone” is somewhat of a misnomer because, although a flat bone is typically thin, it is also often curved. Examples include the cranial (skull) bones, the scapulae (shoulder blades), the sternum (breastbone), and the ribs. Flat bones serve as points of attachment for muscles and often protect internal organs.
- Irregular Bones – An irregular bone is one that does not have any easily characterized shape and therefore does not fit any other classification. These bones tend to have more complex shapes, like the vertebrae that support the spinal cord and protect it from compressive forces. Many facial bones, particularly the ones containing sinuses, are classified as irregular bones.
- Sesamoid Bones – A sesamoid bone is a small, round bone that, as the name suggests, is shaped like a sesame seed. These bones form in tendons (the sheaths of tissue that connect bones to muscles) where a great deal of pressure is generated in a joint. The sesamoid bones protect tendons by helping them overcome compressive forces. Sesamoid bones vary in number and placement from person to person but are typically found in tendons associated with the feet, hands, and knees. The patellae (singular = patella) are the only sesamoid bones found in common with every person.
Bone Structure
Bone tissue (osseous tissue) differs greatly from other tissues in the body. Bone is hard and many of its functions depend on that characteristic hardness. Later discussions in this chapter will show that bone is also dynamic in that its shape adjusts to accommodate stresses. This section will examine the gross anatomy of bone first and then move on to its histology.
Gross Anatomy of Bone
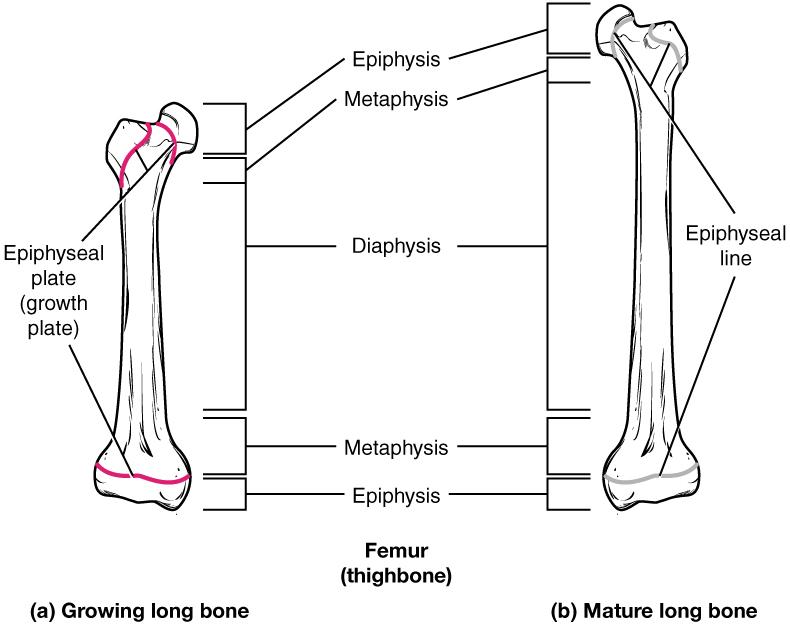
The structure of a long bone allows for the best visualization of all of the parts of a bone (Figure 4.2). A long bone has two parts: the diaphysis and the epiphysis. The diaphysis is the tubular shaft that runs between the proximal and distal ends of the bone. The hollow region in the diaphysis is called the medullary cavity, which is filled with yellow marrow. The walls of the diaphysis are composed of dense and hard compact bone.
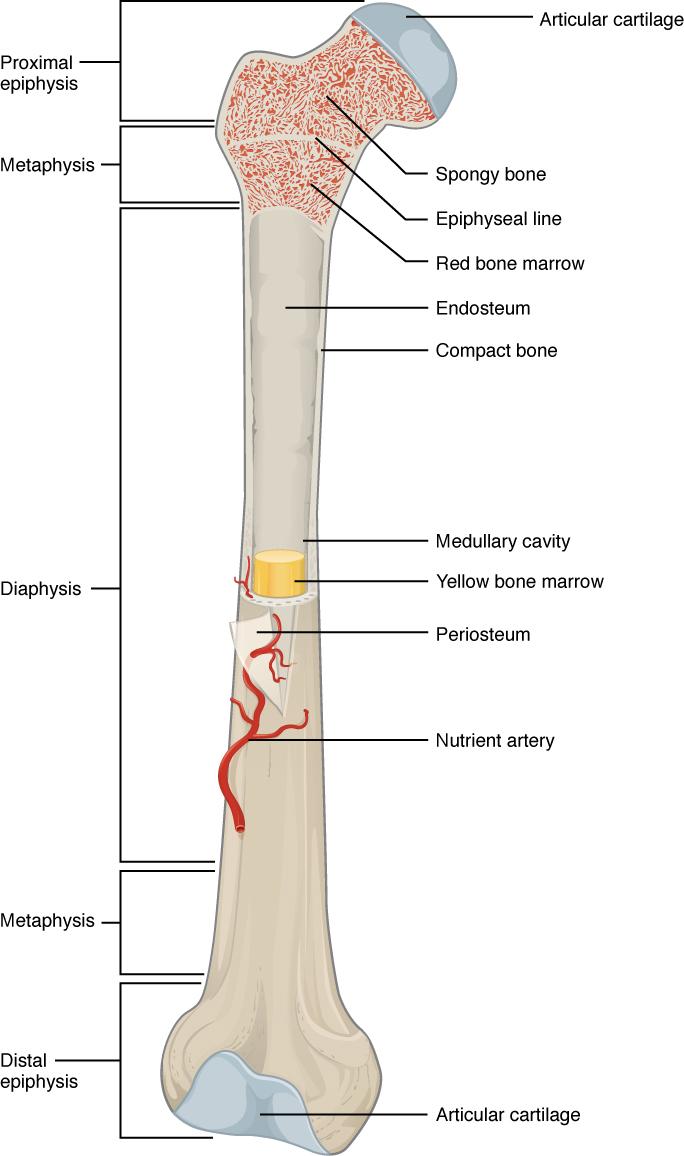
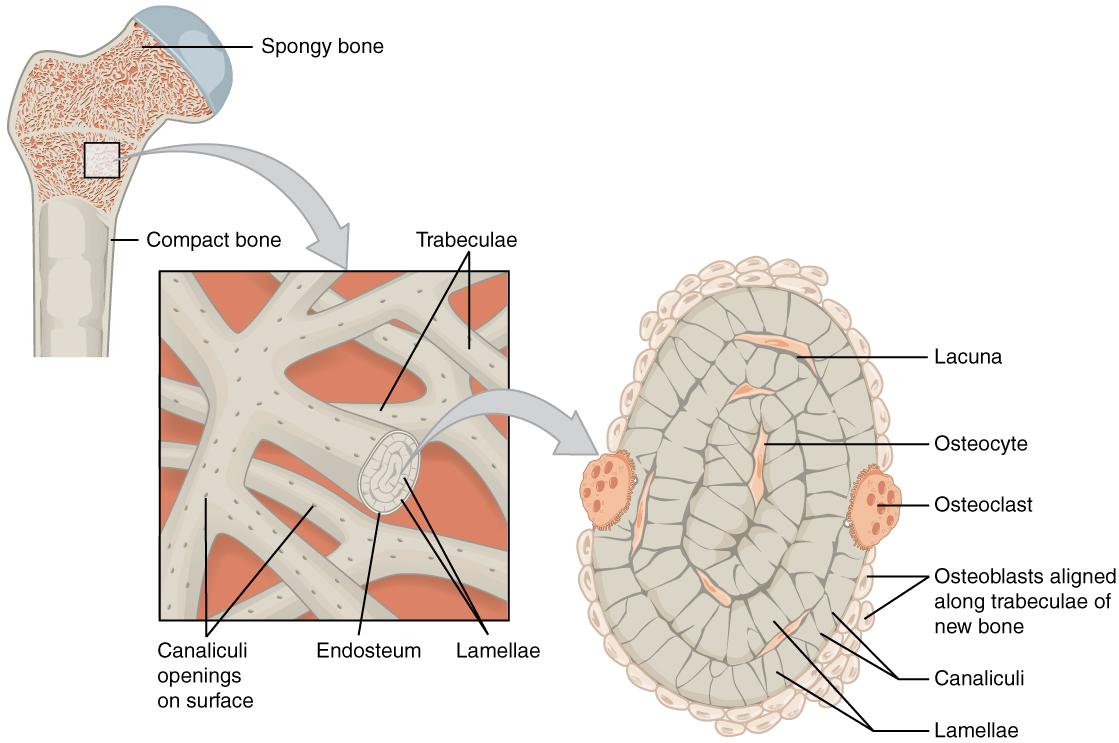
The wider section at each end of the bone is called the epiphysis (plural = epiphyses), which is filled with spongy bone. Red marrow fills the spaces in the spongy bone (Figure 4.3). Each epiphysis meets the diaphysis at the metaphysis, the narrow area that contains the epiphyseal plate (growth plate), a layer of hyaline (transparent) cartilage in a growing bone. When the bone stops growing in early adulthood (approximately 18–21 years), the cartilage is replaced by osseous tissue and the epiphyseal plate becomes an epiphyseal line.
The medullary cavity has a delicate membranous lining called the endosteum (end- = “inside”; oste- = “bone”), where bone growth, repair, and remodeling occur. The outer surface of the bone is covered with a fibrous membrane called the periosteum (peri– = “around” or “surrounding”). The periosteum contains blood vessels, nerves, and lymphatic vessels that nourish compact bone. Tendons and ligaments also attach to bones at the periosteum. The periosteum covers the entire outer surface except where the epiphyses meet other bones to form joints. In this region, the epiphyses are covered with articular cartilage, a thin layer of cartilage that reduces friction and acts as a shock absorber.
Flat bones, like those of the cranium, consist of a layer of spongy bone, lined on either side by a layer of compact bone. The two layers of compact bone and the interior spongy bone work together to protect the internal organs. If the outer layer of a cranial bone fractures, the brain is still protected by the intact inner layer.
Bone Cells and Tissue
Bone contains a relatively small number of cells entrenched in a matrix of collagen fibers that provide a surface for inorganic salt crystals to adhere. These salt crystals form when calcium phosphate and calcium carbonate combine to create hydroxyapatite, which incorporates other inorganic salts like magnesium hydroxide, fluoride, and sulfate as it crystallizes, or calcifies, on the collagen fibers. The hydroxyapatite crystals give bones their hardness and strength, while the collagen fibers give them flexibility so that they are not brittle.
Although bone cells compose a small amount of the bone volume, they are crucial to the function of bones. Four types of cells are found within bone tissue: osteoblasts, osteocytes, osteogenic cells, and osteoclasts.
The osteoblast is the bone cell responsible for forming new bone and is found in the growing portions of bone, including the periosteum and endosteum (Figure 4.4). Osteoblasts, which do not divide, synthesize and secrete the collagen matrix and calcium salts. As the secreted matrix surrounding the osteoblast calcifies, the osteoblast become trapped within it; as a result, it changes in structure and becomes an osteocyte, the primary cell of mature bone and the most common type of bone cell. Each osteocyte is located in a space called a lacuna and is surrounded by bone tissue. Osteocytes maintain the mineral concentration of the matrix via the secretion of enzymes. Like osteoblasts, osteocytes lack mitotic activity. They can communicate with each other and receive nutrients via long cytoplasmic processes that extend through canaliculi (singular = canaliculus), channels within the bone matrix.
If osteoblasts and osteocytes are incapable of mitosis, then how are they replenished when old ones die? The answer lies in the properties of a third category of bone cells—the osteogenic cell. These osteogenic cells are undifferentiated with high mitotic activity and they are the only bone cells that divide. Immature osteogenic cells are found in the deep layers of the periosteum and the marrow. They differentiate and develop into osteoblasts.
The dynamic nature of bone means that new tissue is constantly formed, and old, injured, or unnecessary bone is dissolved for repair or for calcium release. The cell responsible for bone resorption, or breakdown, is the osteoclast. They are found on bone surfaces, are multinucleated, and originate from monocytes and macrophages, two types of white blood cells, not from osteogenic cells. Osteoclasts are continually breaking down old bone while osteoblasts are continually forming new bone. The ongoing balance between osteoblasts and osteoclasts is responsible for the constant but subtle reshaping of bone.
Compact and Spongy Bone
The differences between compact and spongy bone are best explored via their histology. Most bones contain compact and spongy osseous tissue, but their distribution and concentration vary based on the bone’s overall function. Compact bone is dense so that it can withstand compressive forces, while spongy (cancellous) bone has open spaces and supports shifts in weight distribution.
Compact Bone
Compact bone is the denser, stronger of the two types of bone tissue (Figure 4.5). It can be found under the periosteum and in the diaphyses of long bones, where it provides support and protection.
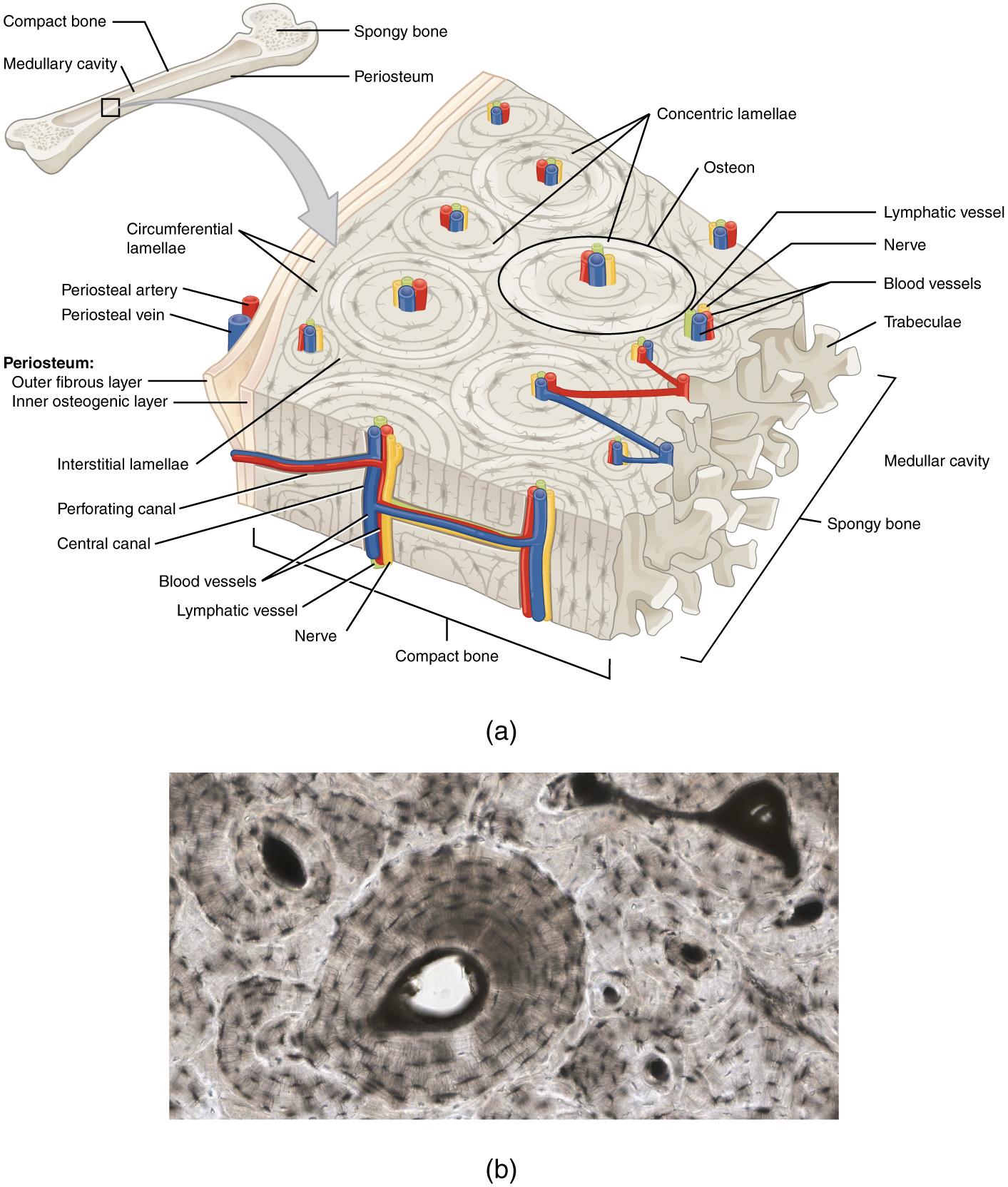
The microscopic structural unit of compact bone is called an osteon, or Haversian system. Each osteon is composed of concentric rings of calcified matrix called lamellae (singular = lamella). Running down the center of each osteon is the central canal, or Haversian canal, which contains blood vessels, nerves, and lymphatic vessels. These vessels and nerves branch off at right angles through a perforating canal, also known as Volkmann’s canals, to extend to the periosteum and endosteum.
The osteocytes are located inside spaces called lacunae (singular = lacuna), found at the borders of adjacent lamellae. Canaliculi connect with the canaliculi of other lacunae and eventually with the central canal. This system allows nutrients to be transported to the osteocytes and wastes to be removed from them.
Spongy Bone
Like compact bone, spongy bone, also known as cancellous bone, contains osteocytes, but they are not arranged in concentric circles. Instead, the osteocytes are found in a lattice-like network of matrix spikes called trabeculae (singular = trabecula) (Figure 4.6). The trabeculae may appear to be a random network, but each trabecula forms along lines of stress to provide strength to the bone. The spaces of the trabeculated network provide balance to the dense and heavy compact bone by making bones lighter so that muscles can move them more easily. In addition, the spaces in some spongy bones contain red marrow, protected by the trabeculae, where hematopoiesis occurs.
How Bones Grow in Length
The epiphyseal plate is the area of growth in a long bone. It is a layer of hyaline cartilage where ossification occurs in immature bones. On the epiphyseal side of the epiphyseal plate, cartilage is formed. On the diaphyseal side, cartilage is ossified, and the diaphysis grows in length. The epiphyseal plate is composed of four zones of cells and activity (Figure 4.7). The reserve zone (zone of resting cartilage) is the region closest to the epiphyseal end of the plate and contains small chondrocytes within the matrix. These chondrocytes do not participate in bone growth but secure the epiphyseal plate to the osseous tissue of the epiphysis.
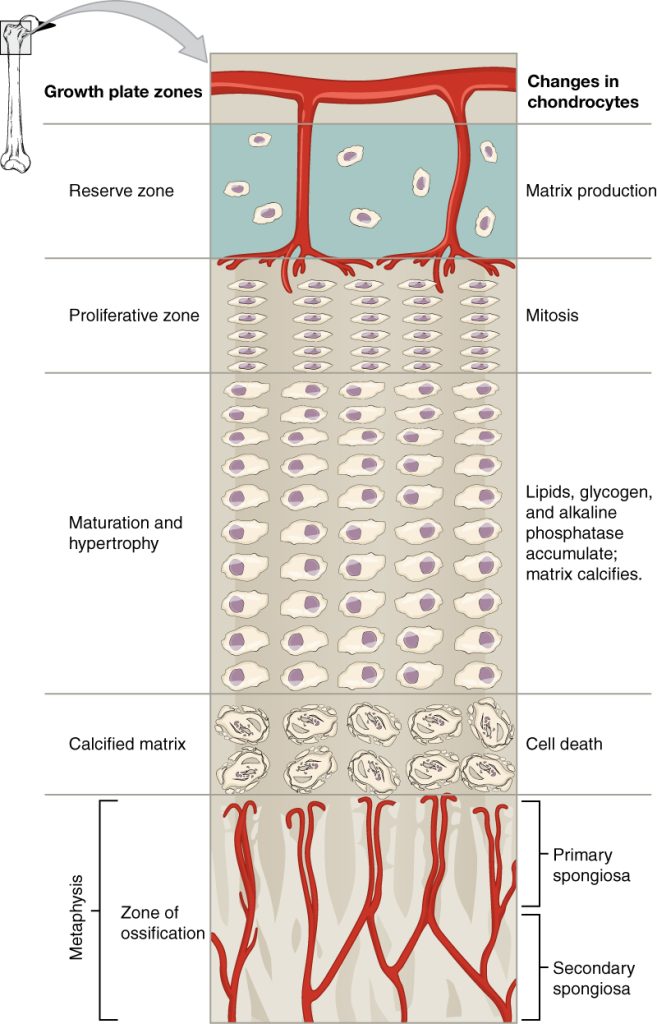
The proliferative zone (zone of proliferating cartilage) is the next layer toward the diaphysis and contains stacks of slightly larger chondrocytes. It makes new chondrocytes (via mitosis) to replace those that die at the diaphyseal end of the plate. Chondrocytes in the next layer, the zone of maturation and hypertrophy (zone of hypertrophic cartilage), are older and larger than those in the proliferative zone. The more mature cells are situated closer to the diaphyseal end of the plate. The longitudinal growth of bone is a result of cellular division in the proliferative zone and the maturation of cells in the zone of maturation and hypertrophy.
Most of the chondrocytes in the zone of calcified matrix (zone of calcified cartilage), the zone closest to the diaphysis, are dead because the matrix around them has calcified. Capillaries and osteoblasts from the diaphysis penetrate this zone, and the osteoblasts secrete bone tissue on the remaining calcified cartilage. Thus, the zone of calcified matrix connects the epiphyseal plate to the diaphysis. A bone grows in length when osseous tissue is added to the diaphysis.
Bones continue to grow in length until early adulthood. The rate of growth is controlled by hormones, which will be discussed later. When the chondrocytes in the epiphyseal plate cease their proliferation and bone replaces the cartilage, longitudinal growth stops. All that remains of the epiphyseal plate is the epiphyseal line (Figure 4.8).
Divisions of the Skeletal System
The skeletal system includes all of the bones, cartilages, and ligaments of the body that support and give shape to the body and body structures. The skeleton consists of the bones of the body. For adults, there are 206 bones in the skeleton. Younger individuals have higher numbers of bones because some bones fuse together during childhood and adolescence to form an adult bone. The primary functions of the skeleton are to provide a rigid, internal structure that can support the weight of the body against the force of gravity, and to provide a structure upon which muscles can act to produce movements of the body. The lower portion of the skeleton is specialized for stability during walking or running. In contrast, the upper skeleton has greater mobility and ranges of motion, features that allow you to lift and carry objects or turn your head and trunk.
In addition to providing for support and movements of the body, the skeleton has protective and storage functions. It protects the internal organs, including the brain, spinal cord, heart, lungs, and pelvic organs. The bones of the skeleton serve as the primary storage site for important minerals such as calcium and phosphate. The bone marrow found within bones stores fat and houses the blood-cell producing tissue of the body.
The skeleton is subdivided into two major divisions—the axial and appendicular.
The Axial Skeleton
The skeleton is subdivided into two major divisions—the axial and appendicular. The axial skeleton forms the vertical, central axis of the body and includes all bones of the head, neck, chest, and back (Figure 4.9). It serves to protect the brain, spinal cord, heart, and lungs. It also serves as the attachment site for muscles that move the head, neck, and back, and for muscles that act across the shoulder and hip joints to move their corresponding limbs.
The axial skeleton of the adult consists of 80 bones, including the skull, the vertebral column, and the thoracic cage. The skull is formed by 22 bones. Also associated with the head are an additional seven bones, including the hyoid bone and the ear ossicles (three small bones found in each middle ear). The vertebral column consists of 24 bones, each called a vertebra, plus the sacrum and coccyx. The thoracic cage includes the 12 pairs of ribs, and the sternum, the flattened bone of the anterior chest.
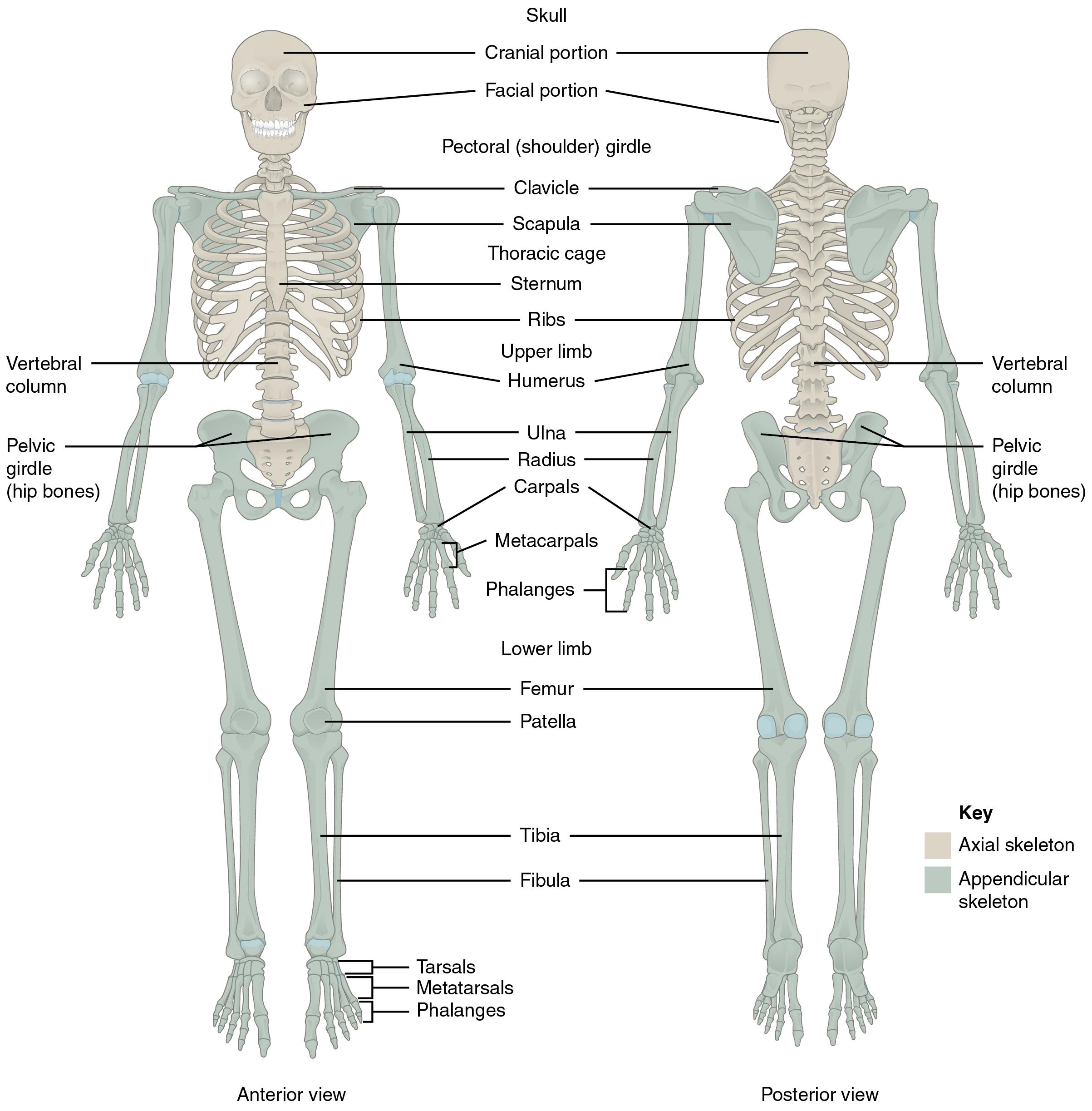
The Appendicular Skeleton
The appendicular skeleton includes all bones of the upper and lower limbs, plus the bones that attach each limb to the axial skeleton. There are 126 bones in the appendicular skeleton of an adult. The bones of the appendicular skeleton are covered in the next chapter.
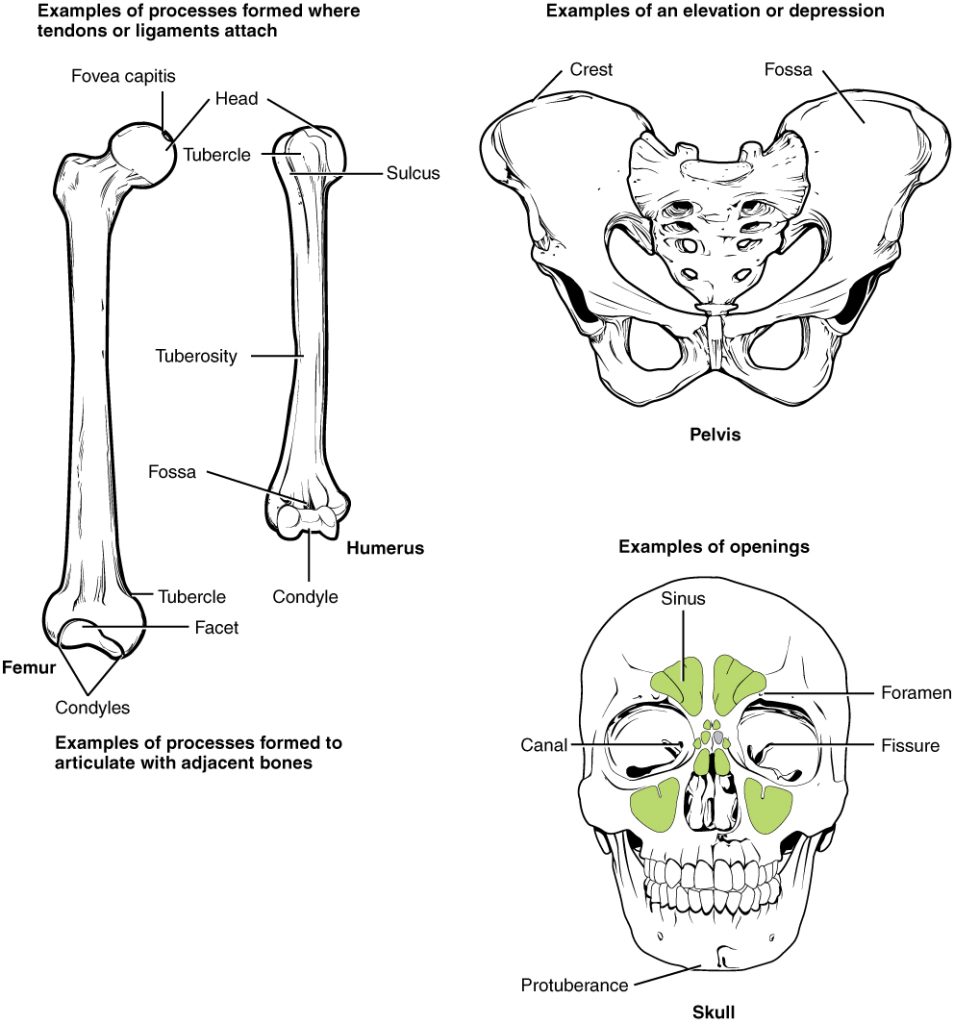
Bone Markings
Before we start learning the morphology of individual bones, you should familiarize yourself with the general terms used to describe bone features. The surface features of bones vary considerably, depending on the function and location in the body. There are three general classes of bone markings: (1) articulations, (2) projections, and (3) holes. As the name implies, an articulation is where two bone surfaces come together (articulus = “joint”). These surfaces tend to conform to one another, such as one being rounded and the other cupped, to facilitate the function of the articulation. A projection is an area of a bone that projects above the surface of the bone. These are the attachment points for tendons and ligaments. In general, their size and shape is an indication of the forces exerted through the attachment to the bone. A hole is an opening or groove in the bone that allows blood vessels and nerves to enter the bone. As with the other markings, their size and shape reflect the size of the vessels and nerves that penetrate the bone at these points.
Commonly used terms for bone markings are illustrated in Figure 4.10 and described in Table 4.1.
| Marking | Description | Example |
|---|---|---|
| Articulations | Where two bones meet | Knee joint |
| Head | Prominent rounded surface | Head of femur |
| Facet | Flat surface | Vertebrae |
| Condyle | Rounded surface | Occipital condyles |
| Projections | Raised markings | Spinous process of the vertebrae |
| Protuberance | Protruding | Chin |
| Process | Prominence feature | Transverse process of vertebra |
| Spine | Sharp process | Ischial spine |
| Tubercle | Small, rounded process | Tubercle of humerus |
| Tuberosity | Rough surface | Deltoid tuberosity |
| Line | Slight, elongated ridge | Temporal lines of the parietal bones |
| Crest | Ridge | Iliac crest |
| Holes | Holes and depressions | Foramen (holes through which blood vessels can pass through) |
| Fossa | Elongated basin | Mandibular fossa |
| Fovea | Small pit | Fovea capitis on the head of the femur |
| Sulcus | Groove | Sigmoid sulcus of the temporal bones |
| Canal | Passage in bone | Auditory canal |
| Fissure | Slit through bone | Auricular fissure |
| Foramen | Hole through bone | Foramen magnum in the occipital bone |
| Meatus | Opening into canal | External auditory meatus |
| Sinus | Air-filled space in bone | Nasal sinus |
Table 4.1 Bone Markings
The Skull
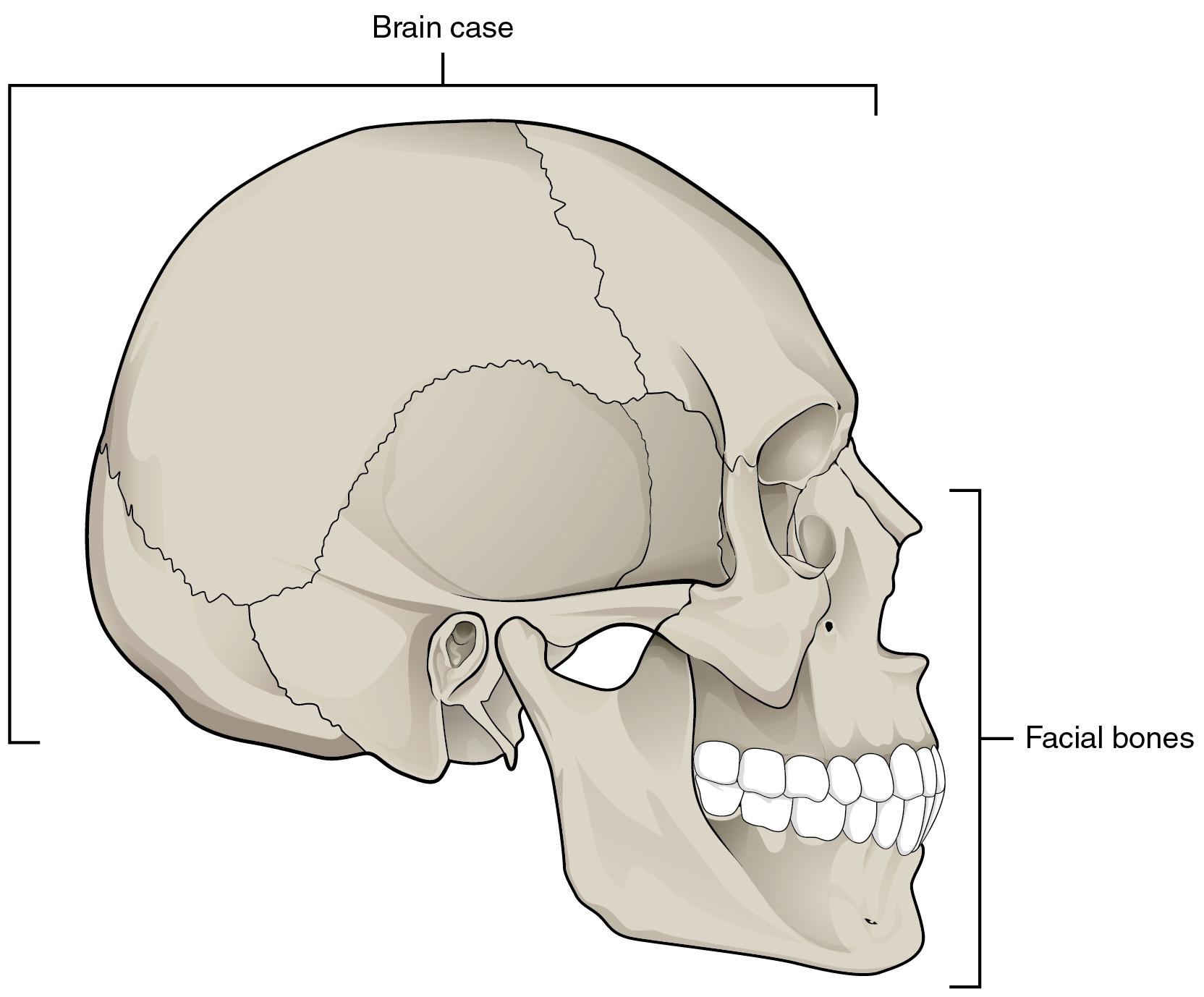
The cranium (skull) is the skeletal structure of the head that supports the face and protects the brain. It is subdivided into the facial bones and the brain case, or neurocranium (Figure 4.11). The facial bones underlie the facial structures, form the nasal cavity, enclose the eyeballs, and support the teeth of the upper and lower jaws. The rounded brain case surrounds and protects the brain and houses the middle and inner ear structures.
In the adult, the skull consists of 22 individual bones, 21 of which are immobile and united into a single unit. The 22nd bone is the mandible (lower jaw), which is the only moveable bone of the skull.
Anterior View of Skull
The anterior skull consists of the facial bones and provides the bony support for the eyes and structures of the face. This view of the skull is dominated by the openings of the orbits and the nasal cavity. Also seen are the upper and lower jaws, with their respective teeth (Figure 4.12).
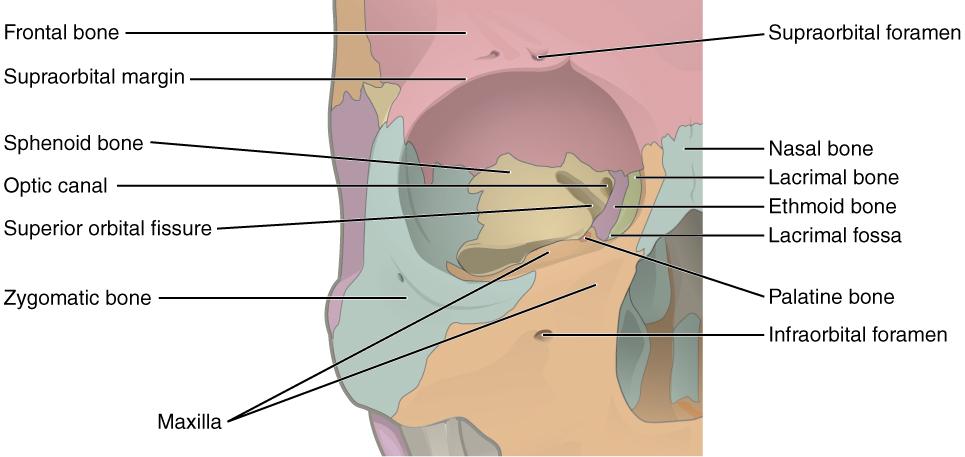
The orbit is the bony socket that houses the eyeball and muscles that move the eyeball or open the upper eyelid. The upper margin of the anterior orbit is the supraorbital margin. Located near the midpoint of the supraorbital margin is a small opening called the supraorbital foramen. This provides for passage of a sensory nerve to the skin of the forehead. Below the orbit is the infraorbital foramen, which is the point of emergence for a sensory nerve that supplies the anterior face below the orbit.
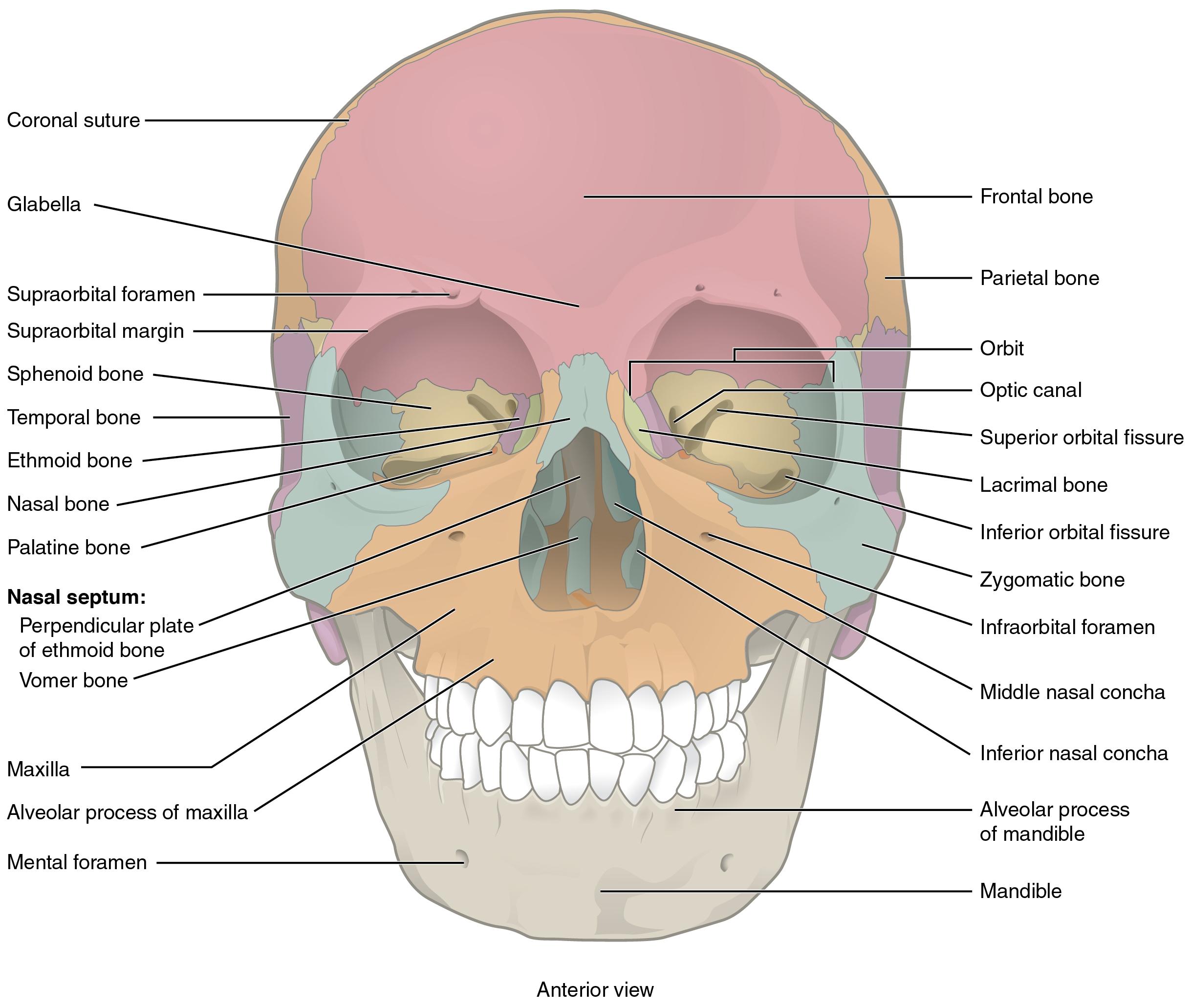
Inside the nasal area of the skull, the nasal cavity is divided into halves by the nasal septum. The upper portion of the nasal septum is formed by the perpendicular plate of the ethmoid bone and the lower portion is the vomer bone. Each side of the nasal cavity is triangular in shape, with a broad inferior space that narrows superiorly. When looking into the nasal cavity from the front of the skull, two bony plates are seen projecting from each lateral wall. The larger of these is the inferior nasal concha, an independent bone of the skull. Located above the inferior concha are the middle nasal concha and superior nasal concha, both of which are part of the ethmoid bone.
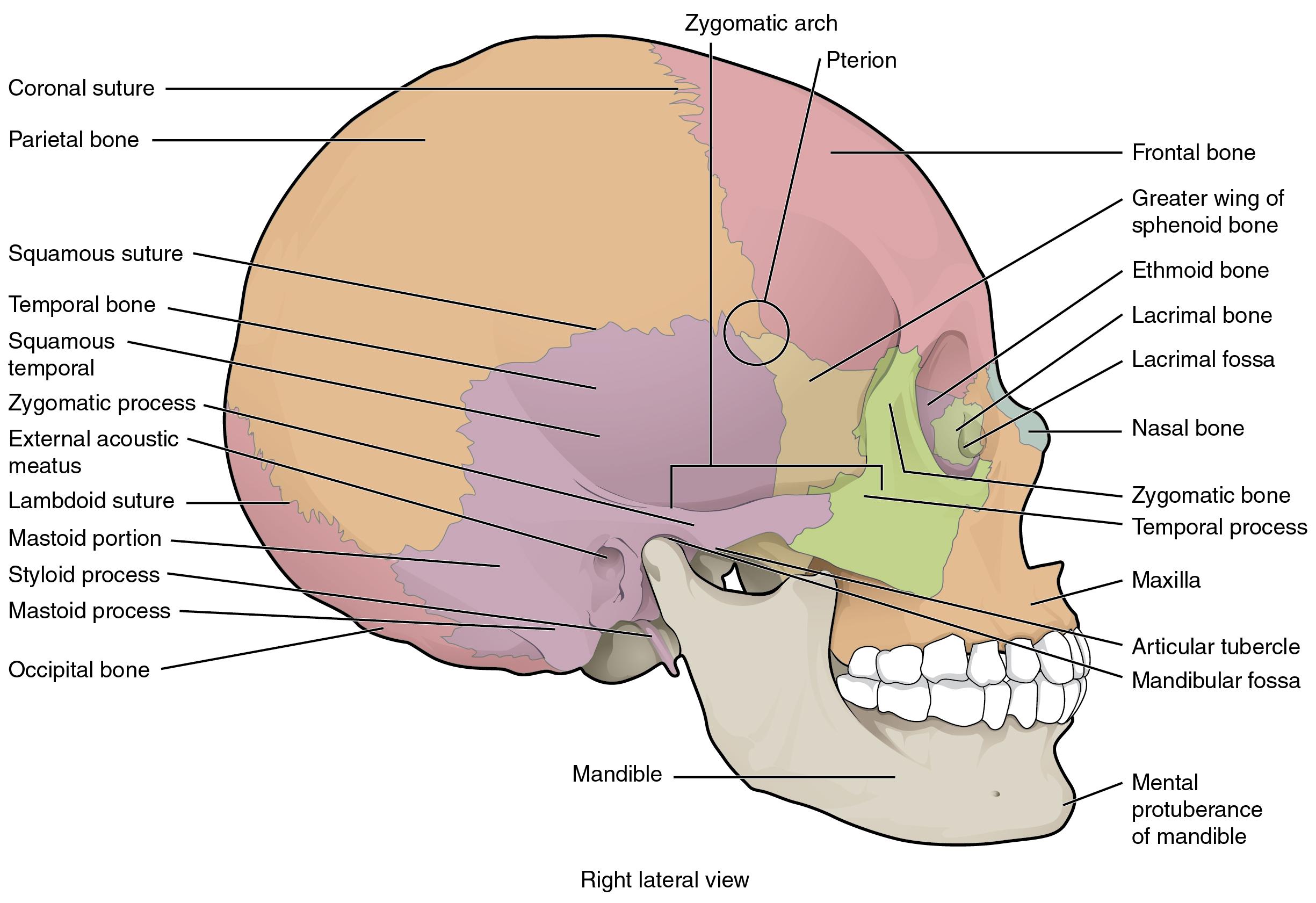
Lateral View of Skull
A view of the lateral skull is dominated by the large, rounded brain case above and the upper and lower jaws with their teeth below (Figure 4.13). Separating these areas is the bridge of bone called the zygomatic arch. The zygomatic arch is the bony arch on the side of the skull that spans from the area of the cheek to just above the ear canal. It is formed by the junction of processes coming from two bones: the zygomatic and temporal bones.
Bones of the Brain Case
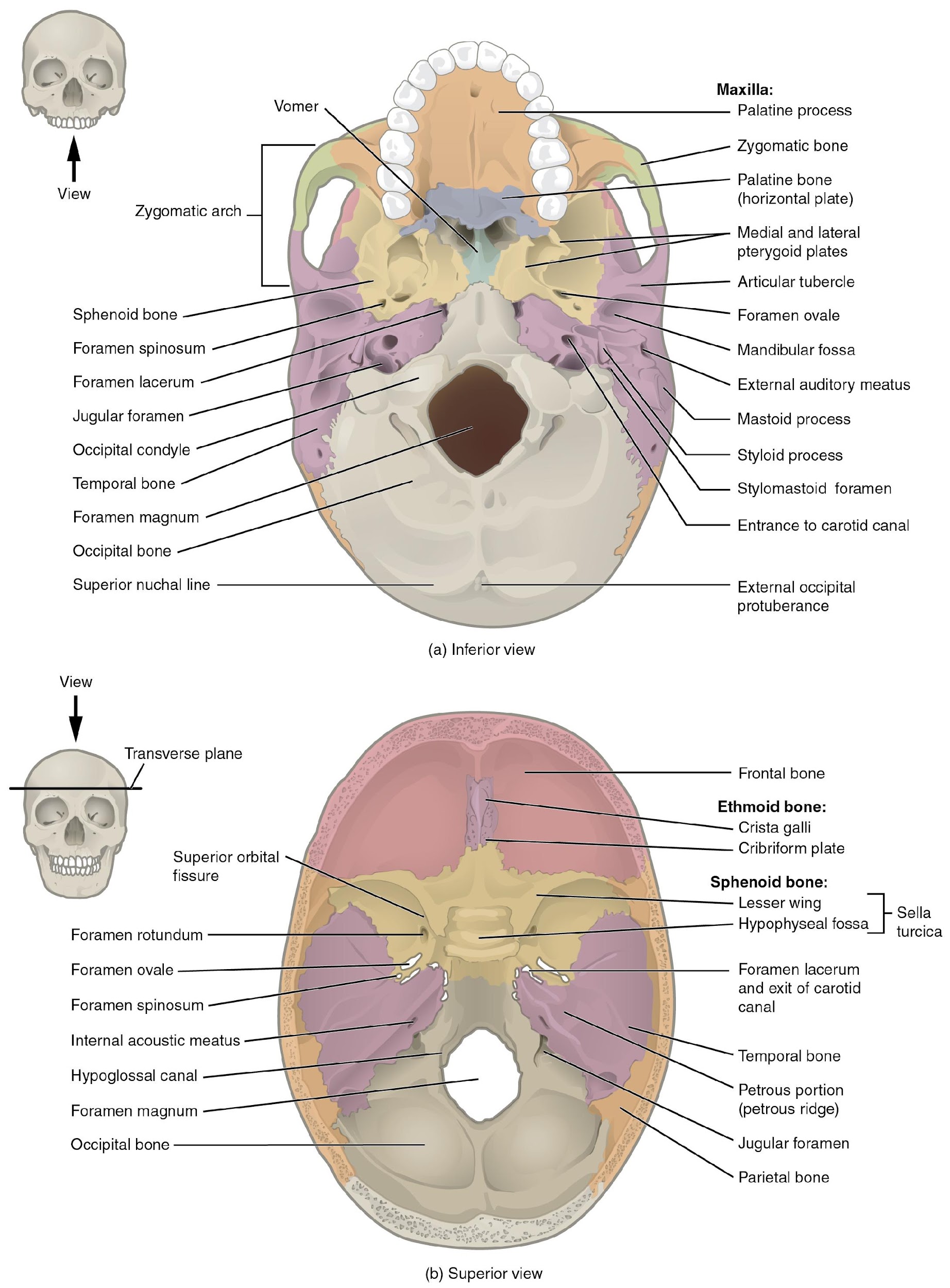
The brain case contains and protects the brain. The interior space that is almost completely occupied by the brain is called the cranial cavity. This cavity is bounded superiorly by the rounded top of the skull, and the lateral and posterior sides of the skull. The bones that form the top and sides of the brain case are usually referred to as the “flat” bones of the skull. The floor of the brain case is referred to as the base of the skull. This is a complex area that varies in depth and has numerous openings for the passage of cranial nerves, blood vessels, and the spinal cord.
The brain case consists of eight bones. These include the paired parietal and temporal bones, plus the unpaired frontal, occipital, sphenoid, and ethmoid bones.
Parietal Bone
The parietal bone forms most of the upper lateral side of the skull (see Figure 4.13). These are paired bones, with the right and left parietal bones joining together at the top of the skull. Each parietal bone is also bounded anteriorly by the frontal bone, inferiorly by the temporal bone, and posteriorly by the occipital bone.
Temporal Bone
The temporal bone forms the lower lateral side of the skull (see Figure 4.13). Common wisdom has it that the temporal bone (temporal = “time”) is so named because this area of the head (the temple) is where hair typically first turns gray, indicating the passage of time.
The temporal bone has a complex morphology. Some of the important landmarks of the temporal bone, as shown in Figures 4.13-4.14, include the following:
- External acoustic meatus (ear canal)—This is the large opening on the lateral side of the skull that is associated with the ear. It leads to the interior of the temporal bone, where the middle and inner ears are housed.
- Internal acoustic meatus—This opening is located inside the cranial cavity, on the medial side of the petrous ridge. It connects to the middle and inner ear cavities of the temporal bone.
- Mandibular fossa—This is the deep, oval-shaped depression located on the external base of the skull, just in front of the external acoustic meatus. The mandible (lower jaw) joins with the skull at this site as part of the temporomandibular joint, which allows for movements of the mandible during opening and closing of the mouth.
- Mastoid process – This is a large prominence projecting from the posterior and inferior region of the temporal bone. It is a muscle attachment site and can easily be felt on the side of the head just behind your earlobe.
- Styloid process—Posterior to the mandibular fossa on the external base of the skull is an elongated, downward bony projection called the styloid process, so named because of its resemblance to a stylus (a pen or writing tool). This structure serves as an attachment site for several small muscles and for a ligament that supports the hyoid bone of the neck.
- Carotid canal—The carotid canal is a zig-zag shaped tunnel that provides passage through the base of the skull for one of the major arteries that supplies the brain. Its entrance is located on the outside base of the skull, anteromedial to the styloid process. The canal then runs anteromedially within the bony base of the skull, and then turns upward to its exit in the floor of the middle cranial cavity, above the foramen lacerum.
Frontal Bone
The frontal bone is the single bone that forms the forehead. At its anterior midline, between the eyebrows, there is a slight depression called the glabella (see Figure 4.12). The frontal bone also forms the supraorbital margin of the orbit. Near the middle of this margin, is the supraorbital foramen, the opening that provides passage for a sensory nerve to the forehead. The frontal bone is thickened just above each supraorbital margin, forming rounded brow ridges. These are located just behind your eyebrows and vary in size among individuals, although they are generally larger in males. Inside the cranial cavity, the frontal bone extends posteriorly. This flattened region forms both the roof of the orbit below and the floor of the anterior cranial cavity above (see Figure 4.14).
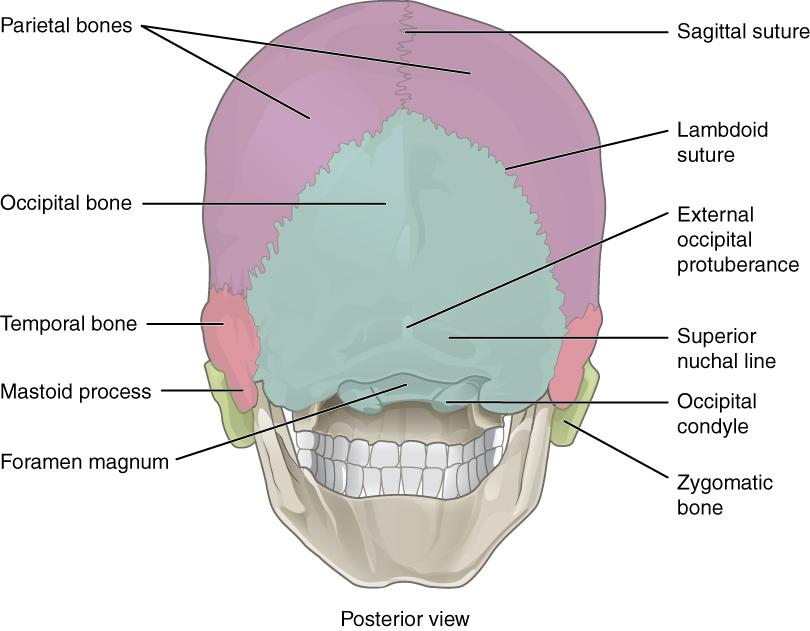
Occipital Bone
The occipital bone is the single bone that forms the posterior skull and posterior base of the cranial cavity (Figure 4.15; see also Figure 4.14). On the base of the skull, the occipital bone contains the large opening of the foramen magnum, which allows for passage of the spinal cord as it exits the skull. On either side of the foramen magnum is an oval-shaped occipital condyle. These condyles form joints with the first cervical vertebra (C1) and thus support the skull on top of the vertebral column.
Sphenoid Bone
The sphenoid bone is a single, complex bone of the central skull (best seen in internal view, Figure 4.14). It serves as a “keystone” bone, because it joins with almost every other bone of the skull. The sphenoid forms much of the base of the central skull and also extends laterally to contribute to the sides of the skull (see Figure 4.13). Inside the cranial cavity, the sella turcica (“Turkish saddle”) is located centrally. This bony region of the sphenoid bone is named for its resemblance to the horse saddles used by the Ottoman Turks, with a high back and a tall front. The rounded depression in the floor of the sella turcica houses the pea-sized pituitary (hypophyseal) gland in the hypophyseal fossa. Running through the sphenoid are two optic canals, which are the passageways for the optic nerves from the orbits into the internal cranial cavity.
Ethmoid Bone
The ethmoid bone is a single, midline bone that forms the roof and lateral walls of the upper nasal cavity, the superior and middle nasal concha (thin, curved projections that extend into the nasal cavity), the upper portion of the nasal septum, and contributes to the medial wall of the orbit (see Figures 4.13-4.14). On the interior of the skull, the ethmoid also forms a portion of the floor of the anterior cranial cavity.
In the cranial cavity, the ethmoid bone forms a small area at the midline in the anterior floor, notched into the frontal bone. This portion of the ethmoid bone consists of two parts, the crista galli and cribriform plates. The crista galli (“rooster’s comb or crest”) is a small upward bony projection located at the midline. It functions as an anterior attachment point for one of the covering layers of the brain. To either side of the crista galli is the cribriform plate (cribrum = “sieve”), a small, flattened area with numerous small openings termed olfactory foramina. Small nerve branches from the olfactory areas of the nasal cavity pass through these openings to enter the brain.
Facial Bones of the Skull
The facial bones of the skull form the upper and lower jaws, and contribute to the nose, nasal cavity and nasal septum, and the orbit. The facial bones include 14 bones, with six paired bones and two unpaired bones. The paired bones are the maxilla, palatine, zygomatic, nasal, lacrimal, and inferior nasal conchae bones. The unpaired bones are the vomer and mandible bones.
Maxillary Bone
The maxillary bone, often referred to simply as the maxilla (plural = maxillae), is one of a pair that together form the upper jaw, much of the hard palate, the medial floor of the orbit, and the lateral base of the nose (see Figures 4.12-4.14). The curved, inferior margin of the maxillary bone that forms the upper jaw and contains the upper teeth is the alveolar process of the maxilla. Each tooth is anchored into a deep socket called an alveolus. On the anterior maxilla, just below the orbit, is the infraorbital foramen. This is the point of exit for a sensory nerve that supplies the nose, upper lip, and anterior cheek. On the inferior skull, the palatine process from each maxillary bone can be seen joining together at the midline to form the anterior three-quarters of the hard palate. The hard palate is the bony plate that forms the roof of the mouth and floor of the nasal cavity, separating the oral and nasal cavities.
Palatine Bone
The palatine bone is one of a pair of irregularly shaped bones that contribute small areas to the lateral walls of the nasal cavity and the medial wall of each orbit. The largest region of each of the palatine bone is the horizontal plate. The plates from the right and left palatine bones join together at the midline to form the posterior quarter of the hard palate (see Figure 4.14). Thus, the palatine bones are best seen in an inferior view of the skull and hard palate.
Zygomatic Bone
The zygomatic bone is also known as the cheekbone. Each of the paired zygomatic bones forms much of the lateral wall of the orbit and the lateral-inferior margins of the anterior orbital opening (see Figures 4.12-4.13). The temporal process of the zygomatic bone projects posteriorly, where it forms the anterior portion of the zygomatic arch.
Nasal Bone
The nasal bone is one of two small bones that articulate (join) with each other to form the bony base (bridge) of the nose. They also support the cartilages that form the lateral walls of the nose (see Figure 4.12). These are the bones that are damaged when the nose is broken.
Lacrimal Bone
Each lacrimal bone is a small, rectangular bone that forms the anterior, medial wall of the orbit (see Figure 4.12 and Figure 4.13). The anterior portion of the lacrimal bone forms a shallow depression called the lacrimal fossa, and extending inferiorly from this is the nasolacrimal canal. The lacrimal fluid (tears of the eye), which serves to maintain the moist surface of the eye, drains at the medial corner of the eye into the nasolacrimal canal. This duct then extends downward to open into the nasal cavity, behind the inferior nasal concha. In the nasal cavity, the lacrimal fluid normally drains posteriorly, but with an increased flow of tears due to crying or eye irritation, some fluid will also drain anteriorly, thus causing a runny nose.
Inferior Nasal Conchae
The right and left inferior nasal conchae form a curved bony plate that projects into the nasal cavity space from the lower lateral wall (see Figure 4.12). The inferior concha is the largest of the nasal conchae and can easily be seen when looking into the anterior opening of the nasal cavity.
Vomer Bone
The unpaired vomer bone, often referred to simply as the vomer, is triangular-shaped and forms the posterior-inferior part of the nasal septum (see Figure 4.12). A small portion of the vomer can be seen when looking into the anterior opening of the nasal cavity.
Mandible
The mandible forms the lower jaw and is the only moveable bone of the skull. At the time of birth, the mandible consists of paired right and left bones, but these fuse together during the first year to form the single U-shaped mandible of the adult skull. Each side of the mandible consists of a horizontal body and posteriorly, a vertically oriented ramus of the mandible (ramus = “branch”). The posterior, upwardly projecting process on the ramus on each side of the mandible is the mandibular condyle, which articulates (joins) with the mandibular fossa of the temporal bone (Figure 4.13). Together these articulations form the temporomandibular joint, which allows for opening and closing of the mouth. Like the maxillae, the mandible contains alveoli (sockets) for teeth.
The Orbit
The orbit is the bony socket that houses the eyeball and contains the muscles that move the eyeball or open the upper eyelid. Each orbit is cone-shaped, with a narrow posterior region that widens toward the large anterior opening. To help protect the eye, the bony margins of the anterior opening are thickened and somewhat constricted. The medial walls of the two orbits are parallel to each other but each lateral wall diverges away from the midline at a 45° angle. This divergence provides greater lateral peripheral vision.
The walls of each orbit include contributions from seven skull bones (Figure 4.16). The frontal bone forms the roof and the zygomatic bone forms the lateral wall and lateral floor. The medial floor is primarily formed by the maxilla, with a small contribution from the palatine bone. The ethmoid bone and lacrimal bone make up much of the medial wall and the sphenoid bone forms the posterior orbit.
At the posterior apex of the orbit is the opening of the optic canal, which allows for passage of the optic nerve from the retina to the brain. Lateral to this is the elongated and irregularly shaped superior orbital fissure, which provides passage for the artery that supplies the eyeball, sensory nerves, and the nerves that supply the muscles involved in eye movements.
The Nasal Septum and Nasal Conchae
The nasal septum consists of both bone and cartilage components (Figure 4.13). The upper portion of the septum is formed by the perpendicular plate of the ethmoid bone. The lower and posterior parts of the septum are formed by the triangular-shaped vomer bone. In an anterior view of the skull, the perpendicular plate of the ethmoid bone is easily seen inside the nasal opening as the upper nasal septum, but only a small portion of the vomer is seen as the inferior septum. The anterior nasal septum is formed by the septal cartilage, a flexible plate that fills in the gap between the perpendicular plate of the ethmoid and vomer bones. This cartilage also extends outward into the nose where it separates the right and left nostrils. The septal cartilage is not found in the dry skull.
Attached to the lateral wall on each side of the nasal cavity are the superior, middle, and inferior nasal conchae (singular = concha), which are named for their positions (see Figure 4.13). These are bony plates that curve downward as they project into the space of the nasal cavity. They serve to swirl the incoming air, which helps to warm and moisturize it before the air moves into the delicate air sacs of the lungs. This also allows mucus, secreted by the tissue lining the nasal cavity, to trap incoming dust, pollen, bacteria, and viruses. The largest of the conchae is the inferior nasal concha, which is an independent bone of the skull. The middle concha and the superior conchae, which is the smallest, are both formed by the ethmoid bone. When looking into the anterior nasal opening of the skull, only the inferior and middle conchae can be seen. The small superior nasal concha is well hidden above and behind the middle concha.
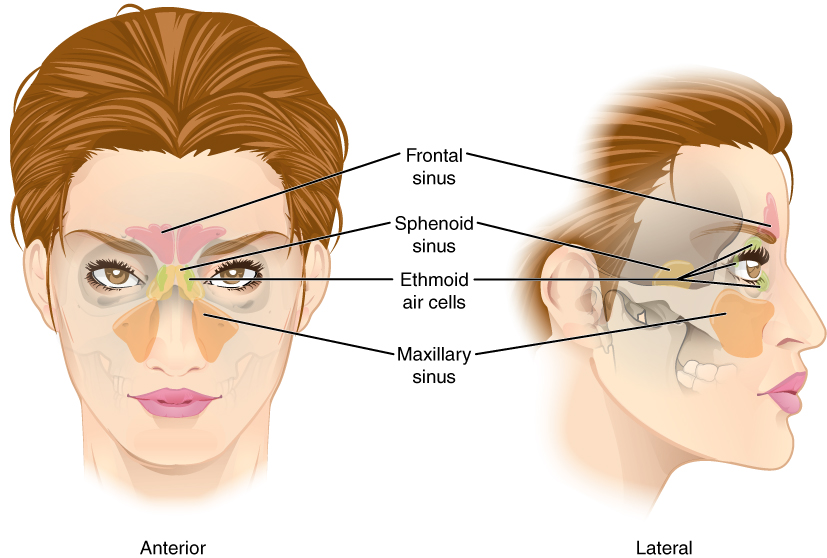
Paranasal Sinuses
The paranasal sinuses are hollow, air-filled spaces located within certain bones of the skull (Figure 4.17). All of the sinuses communicate with the nasal cavity (paranasal = “next to nasal cavity”) and are lined with nasal mucosa. They serve to reduce bone mass and thus lighten the skull, and they also add resonance to the voice. This second feature is most obvious when you have a cold or sinus congestion. These produce swelling of the mucosa and excess mucus production, which can obstruct the narrow passageways between the sinuses and the nasal cavity, causing your voice to sound different to yourself and others. This blockage can also allow the sinuses to fill with fluid, with the resulting pressure producing pain and discomfort.
The paranasal sinuses are named for the skull bone that each occupies. The frontal sinus is located just above the eyebrows, within the frontal bone. The largest sinus is the maxillary sinus. These are paired and located within the right and left maxillary bones, where they occupy the area just below the orbits. The maxillary sinuses are most commonly involved during sinus infections. Because their connection to the nasal cavity is located high on their medial wall, they are difficult to drain. The sphenoid sinus is a single, midline sinus. It is located within the body of the sphenoid bone, just anterior and inferior to the sella turcica, thus making it the most posterior of the paranasal sinuses. The lateral aspects of the ethmoid bone contain multiple small spaces separated by very thin bony walls. Each of these spaces is called an ethmoid air cell. These are located on both sides of the ethmoid bone, between the upper nasal cavity and medial orbit, just behind the superior nasal conchae.
Sutures of the Skull
A suture is an immobile joint between adjacent bones of the skull. The narrow gap between the bones is filled with dense, fibrous connective tissue that unites the bones. The long sutures located between the bones of the brain case are not straight, but instead follow irregular, tightly twisting paths. These twisting lines serve to tightly interlock the adjacent bones, thus adding strength to the skull for brain protection.
The two suture lines seen on the top of the skull are the coronal and sagittal sutures. The coronal suture runs from side to side across the skull, within the coronal plane of section (see Figure 4.13). It joins the frontal bone to the right and left parietal bones. The sagittal suture extends posteriorly from the coronal suture, running along the midline at the top of the skull in the sagittal plane of section (see Figure 4.15). It unites the right and left parietal bones. On the posterior skull, the sagittal suture terminates by joining the lambdoid (lambdoidal) suture (see Figure 4.15). The lambdoid suture extends downward and laterally to either side away from its junction with the sagittal suture. The lambdoid suture joins the occipital bone to the right and left parietal and temporal bones. This suture is named for its upside-down “V” shape, which resembles the capital letter version of the Greek letter lambda (Λ). The squamous suture is located on the lateral skull. It unites the temporal bone with the parietal bone (see Figure 4.13).
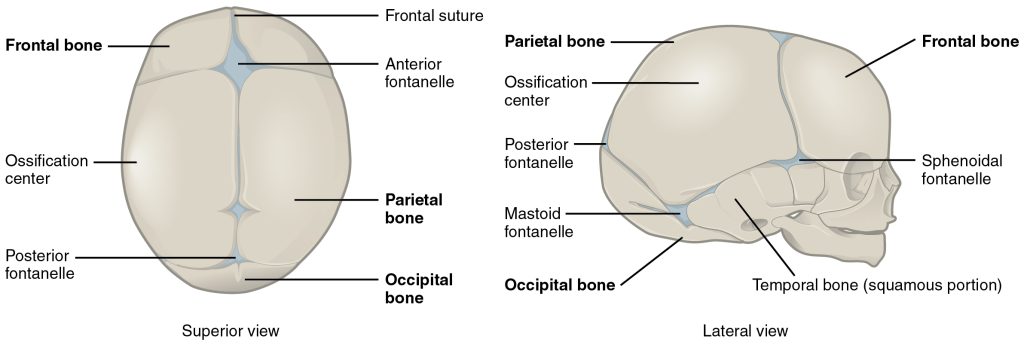
Development of the Skull
The bones of the skull arise from mesenchyme during embryonic development in two different ways. The first mechanism produces the bones that form the top and sides of the brain case. This involves the local accumulation of mesenchymal cells at the site of the future bone. These cells then differentiate directly into bone producing cells, which form the skull bones through the process of intramembranous ossification. As the brain case bones grow in the fetal skull, they remain separated from each other by large areas of dense connective tissue, each of which is called a fontanelle (Figure 4.18). The fontanelles are the soft spots on an infant’s head. They are important during birth because these areas allow the skull to change shape as it squeezes through the birth canal. After birth, the fontanelles allow for continued growth and expansion of the skull as the brain enlarges. The largest fontanelle is located on the anterior head, at the junction of the frontal and parietal bones. The fontanelles decrease in size and disappear by age 2. However, the skull bones remained separated from each other at the sutures, which contain dense fibrous connective tissue that unites the adjacent bones. The connective tissue of the sutures allows for continued growth of the skull bones as the brain enlarges during childhood growth.
The second mechanism for bone development in the skull produces the facial bones and floor of the brain case. This also begins with the localized accumulation of mesenchymal cells. However, these cells differentiate into cartilage cells, which produce a hyaline cartilage model of the future bone. As this cartilage model grows, it is gradually converted into bone through the process of endochondral ossification. This is a slow process and the cartilage is not completely converted to bone until the skull achieves its full adult size.
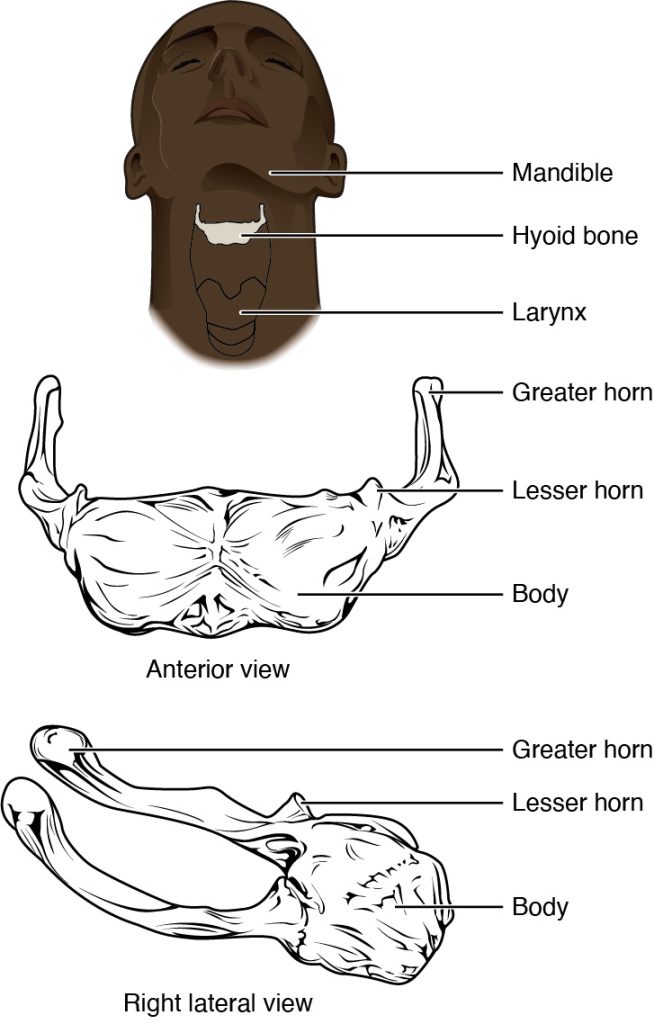
Hyoid Bone
The hyoid bone is an independent bone that does not contact any other bone and thus is not part of the skull (Figure 4.19). It is a small U-shaped bone located in the upper neck near the level of the inferior mandible, with the tips of the “U” pointing posteriorly. The hyoid serves as the base for the tongue above, and is attached to the larynx below and the pharynx posteriorly. The hyoid is held in position by a series of small muscles that attach to it either from above or below. These muscles act to move the hyoid up/down or forward/back. Movements of the hyoid are coordinated with movements of the tongue, larynx, and pharynx during swallowing and speaking.
The Vertebral Column
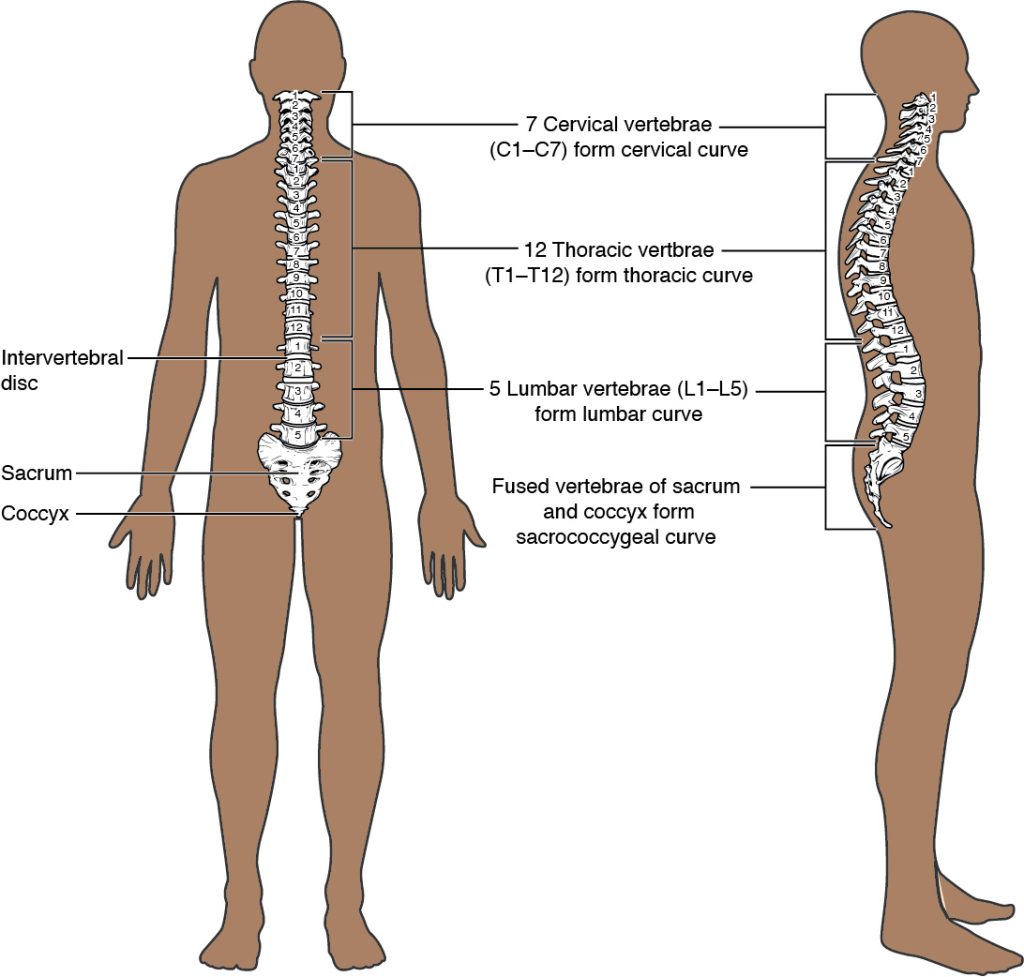
The vertebral column is also known as the spinal column or spine (Figure 4.20). It consists of a sequence of vertebrae (singular = vertebra), each of which is separated and united by an intervertebral disc. Together, the vertebrae and intervertebral discs form the vertebral column. It is a flexible column that supports the head, neck, and body and allows for their movements. It also protects the spinal cord, which passes down the back through openings in the vertebrae.
Regions of the Vertebral Column
The vertebral column originally develops as a series of 33 vertebrae, but this number is eventually reduced to 24 vertebrae, plus the sacrum and coccyx. The vertebral column is subdivided into five regions, with the vertebrae in each area named for that region and numbered in descending order. In the neck, there are seven cervical vertebrae, each designated with the letter “C” followed by its number. Superiorly, the C1 vertebra articulates (forms a joint) with the occipital condyles of the skull. Inferiorly, C1 articulates with the C2 vertebra, and so on. Below these are the 12 thoracic vertebrae, designated T1–T12. The lower back contains the L1–L5 lumbar vertebrae. The single sacrum, which is also part of the pelvis, is formed by the fusion of five sacral vertebrae. Similarly, the coccyx, or tailbone, results from the fusion of four small coccygeal vertebrae. However, the sacral and coccygeal fusions do not start until age 20 and are not completed until middle age.
Curvatures of the Vertebral Column
The adult vertebral column does not form a straight line, but instead has four curvatures along its length (see Figure 4.20). These curves increase the vertebral column’s strength, flexibility, and ability to absorb shock. When the load on the spine is increased, by carrying a heavy backpack for example, the curvatures increase in depth (become more curved) to accommodate the extra weight. They then spring back when the weight is removed. The four adult curvatures are classified as either primary or secondary curvatures. Primary curves are retained from the original fetal curvature, while secondary curvatures develop after birth.
During fetal development, the body is flexed anteriorly into the fetal position, giving the entire vertebral column a single curvature that is concave anteriorly. In the adult, this fetal curvature is retained in two regions of the vertebral column as the thoracic curve, which involves the thoracic vertebrae, and the sacrococcygeal curve, formed by the sacrum and coccyx. Each of these is thus called a primary curve because they are retained from the original fetal curvature of the vertebral column.
A secondary curve develops gradually after birth as the child learns to sit upright, stand, and walk. Secondary curves are concave posteriorly, opposite in direction to the original fetal curvature. The cervical curve of the neck region develops as the infant begins to hold their head upright when sitting. Later, as the child begins to stand and then to walk, the lumbar curve of the lower back develops. In adults, the lumbar curve is generally deeper in females.
General Structure of a Vertebra
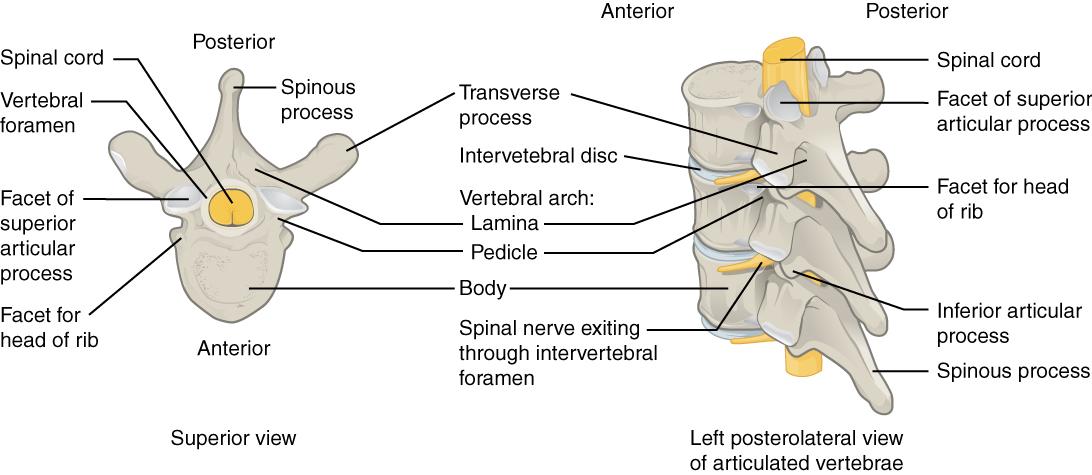
Within the different regions of the vertebral column, vertebrae vary in size and shape, but they all follow a similar structural pattern. A typical vertebra will consist of a body, a vertebral arch, and several processes (Figure 4.21). The body is the anterior portion of each vertebra and is the part that supports the body weight. Because of this, the vertebral bodies progressively increase in size and thickness going down the vertebral column. The bodies of adjacent vertebrae are separated and strongly united by an intervertebral disc. The vertebral arch forms the posterior portion of each vertebra. The large opening between the vertebral arch and body is the vertebral foramen, which contains the spinal cord. In the intact vertebral column, the vertebral foramina of all of the vertebrae align to form the vertebral (spinal) canal, which serves as the bony protection and passageway for the spinal cord down the back. When the vertebrae are aligned together in the vertebral column, notches in the vertebral arches of adjacent vertebrae together form an intervertebral foramen, the opening through which a spinal nerve exits from the vertebral column.
The paired transverse processes laterally and the single spinous process (vertebral spine) projecting posteriorly at the midline of the back serve as important muscle attachment sites. There are also superior and inferior articular processes that articulate with the vertebrae above and below, respectively. These junctions form slightly moveable joints between the adjacent vertebrae. The shape and orientation of the articular processes vary in different regions of the vertebral column and play a major role in determining the type and range of motion available in each region.
The Thoracic Cage
The thoracic cage (rib cage) forms the thorax (chest) portion of the body. It consists of the 12 pairs of ribs with their costal cartilages and the sternum (Figure 4.22). The ribs are anchored posteriorly to the 12 thoracic vertebrae (T1–T12). The thoracic cage protects the heart and lungs.
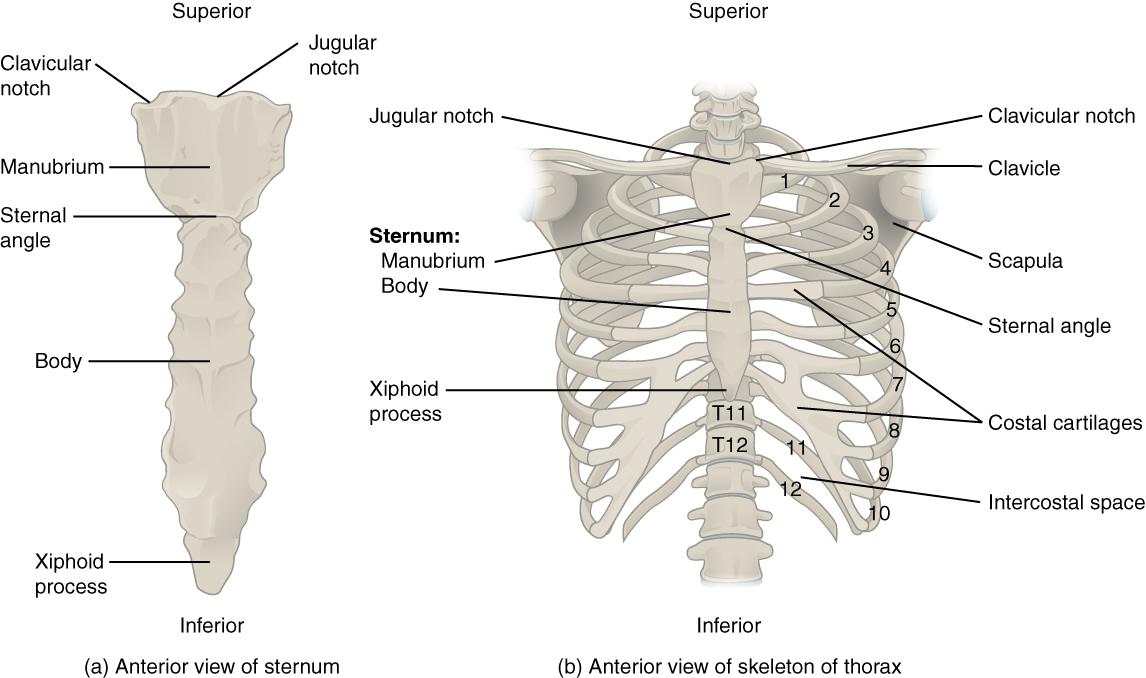
Sternum
The sternum is the elongated bony structure that anchors the anterior thoracic cage. It consists of three parts: the manubrium, body, and xiphoid process. The manubrium is the wider, superior portion of the sternum. The top of the manubrium has a shallow, U-shaped border called the jugular (suprasternal) notch. This can be easily felt at the anterior base of the neck, between the medial ends of the clavicles. The clavicular notch is the shallow depression located on either side at the superior-lateral margins of the manubrium. This is the site of the sternoclavicular joint, between the sternum and clavicle. The first ribs also attach to the manubrium.
The elongated, central portion of the sternum is the body. The manubrium and body join together at the sternal angle, so called because the junction between these two components is not flat, but forms a slight bend. The second rib attaches to the sternum at the sternal angle. Since the first rib is hidden behind the clavicle, the second rib is the highest rib that can be identified by palpation. Thus, the sternal angle and second rib are important landmarks for the identification and counting of the lower ribs. Ribs 3–7 attach to the sternal body.
The inferior tip of the sternum is the xiphoid process. This small structure is cartilaginous early in life, but gradually becomes ossified starting during middle age.
Ribs
Each rib is a curved, flattened bone that contributes to the wall of the thorax. The ribs articulate posteriorly with the T1–T12 thoracic vertebrae, and most attach anteriorly via their costal cartilages to the sternum. There are 12 pairs of ribs. The ribs are numbered 1–12 in accordance with the thoracic vertebrae.
The bony ribs do not extend anteriorly completely around to the sternum. Instead, each rib ends in a costal cartilage. These cartilages are made of hyaline cartilage and can extend for several inches. Most ribs are then attached, either directly or indirectly, to the sternum via their costal cartilage (see Figure 4.22). The ribs are classified into three groups based on their relationship to the sternum:
- Ribs 1–7 are classified as true ribs (vertebrosternal ribs). The costal cartilage from each of these ribs attaches directly to the sternum.
- Ribs 8–12 are called false ribs (vertebrochondral ribs). The costal cartilages from these ribs do not attach directly to the sternum. For ribs 8–10, the costal cartilages are attached to the cartilage of the next higher rib. Thus, the cartilage of rib 10 attaches to the cartilage of rib 9, rib 9 then attaches to rib 8, and rib 8 is attached to rib 7.
- The last two false ribs (11–12) are also called floating ribs (vertebral ribs). These are short ribs that do not attach to the sternum at all. Instead, their small costal cartilages terminate within the musculature of the lateral abdominal wall.
Unless otherwise indicated, this chapter contains material adapted from Anatomy and Physiology (on OpenStax), by Betts, et al. and is used under a a CC BY 4.0 international license. Download and access OpenStax Anatomy and Physiology for free at https://openstax.org/books/anatomy-and-physiology/pages/1-introduction.
