
The Female Reproductive System
Uterine Tubes
The uterine tubes (also called fallopian tubes or oviducts) serve as the conduit of the oocyte from the ovary to the uterus (Figure 1). Each tube is 10–12 centimeters in length and covered by the mesosalpinx, part of the broad ligament.
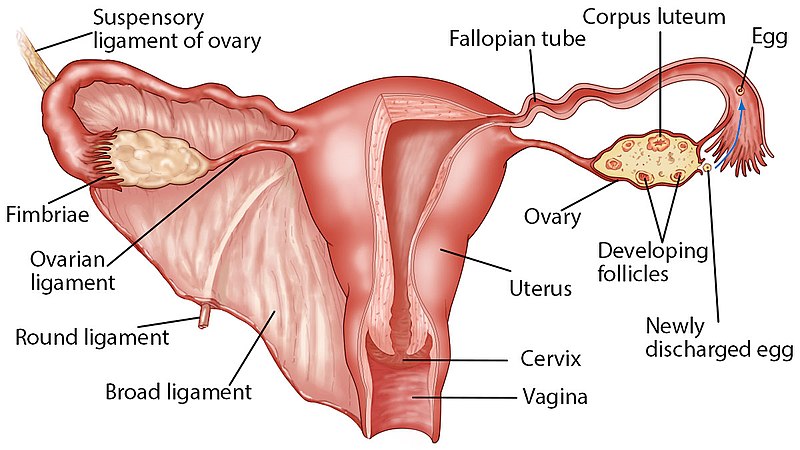
Each of the two uterine tubes is close to, but not directly connected to, the ovary and divided into sections. The lateral distal opening close to the ovary is the infundibulum. The infundibulum flares out with slender, finger-like projections called fimbriae, which capture the released oocyte. Medial to the infundibulum is an extended tube, a region called the ampulla, where fertilization often occurs. Medial to the ampulla is a narrow straight segment, about 1/3 of the entire length of the uterine tube, called the isthmus. The most medial narrow segment of the tubes (interstitial segment) runs through the uterine wall and is continuous with the uterine cavity.
The wall of the uterine tubes consists of three layers:
- an inner epithelial lining mucosa, which facing the lumen of the tubes,
- a middle smooth muscle layer (muscularis mucosa), responsible for peristalsis and rhythmic contraction of the tubes and movement of the released or fertilized egg, and
- an outer serosa layer, connective tissue, covered by peritoneal membrane and the mesosalpinx.
The epithelial lining mucosa consists of two types of cells. Ciliated columnar epithelial cells beat in the direction of the uterus and produce a current that will be critical to moving the oocyte/fertilized egg, and secretory (peg cells) non-ciliated cells provide nourishment and protect the released oocytes or the fertilized embryo.
It usually takes the fertilized egg approximately three days of to travel the length of the uterine tube and reach the lumen of the uterus. Delay in movement may lead to early implantation and ectopic pregnancy.
Function of the Fallopian Tubes
Following ovulation, the secondary oocyte, surrounded by zona pellucida and a few granulosa cells corona radiata, is released into the peritoneal cavity. The nearby uterine tube, either left or right, receives the oocyte. Unlike sperm, oocytes lack flagella and cannot move on their own. High concentrations of estrogen that occur around the time of ovulation induce contractions of the smooth muscle along the length of the uterine tube. These contractions occur every 4 to 8 seconds, and the result is a coordinated movement that sweeps the surface of the ovary and the pelvic cavity, capturing the released egg by the fimbria. Current flowing toward the uterus is generated by coordinated beating of the cilia that line the outside and lumen of the length of the uterine tube. These cilia beat more strongly in response to the high estrogen concentrations that occur around the time of ovulation. As a result of these mechanisms, the oocyte–granulosa cell complex is pulled into the interior of the tube. Once inside, the muscular contractions and beating cilia move the oocyte slowly toward the uterus. When fertilization does occur, the sperm typically meet the egg while it is still moving through the ampulla.
Clinical Correlation
Sepsis and Infertility
The open-ended structure of the uterine tubes can have significant health consequences if bacteria or other contagions enter through the vagina and move through the uterus, into the tubes, and then into the pelvic cavity. If left unchecked, this bacterial infection (sepsis) could quickly become life-threatening.
Cause of infection (Sepsis)
The spread of an infection in this manner is of special concern when unskilled practitioners perform abortions in non-sterile conditions. Sepsis is also associated with sexually transmitted bacterial infections, especially gonorrhea and chlamydia. These STIs increase a woman’s risk for pelvic inflammatory disease (PID), an infection of the uterine tubes or other reproductive organs. Even when resolved, PID can leave scar tissue in the tubes, leading to infertility.
Take Home Message
- The ampulla is the proper place for fertilization to occur.
- Ciliated cells lining the uterine tubes propel the egg in one direction toward uterine cavity.
- The peritoneal cavity is open in females through the open end of the uterine tubes, and can lead to infection and sepsis.
Image Sources
- Figure 1. “Labeled ovary and fallopian tubes” is from Zealthy via Wikimedia Commons, licensed CC BY 4.0.

{kind=link}