
Heredity
Diana Lang; Martha Lally; Suzanne Valentine-French; Laura Overstreet; and Naomi H. Dan Karami
- Define gene, chromosome, and gamete.
- Distinguish between mitosis and meiosis, genotype and phenotype, homozygous and heterozygous, and dominant and recessive.
- Question the assertion that human traits are genetic. Define genotype-environment correlations and genotype-environment interactions, and define epigenetics.
- Differentiate between genetic disorders and chromosomal abnormalities. Describe Trisomy 21.
- Describe the function of genetic counseling.
- Describe human development during the germinal, embryonic, and fetal periods and differentiate between the three periods of development.
- Describe a normal delivery and complications of pregnancy and delivery.
- Predict the risks to prenatal development posed by exposure to teratogens.
- Interpret APGAR scores.
- Discover the sensory abilities and risks of newborns
- Describe adoption and understand the family types
- Understand the after process for communication with the adoption process
- Using appropriate adoption terminology
Next, we will present the birth process and some of the complications that can occur during delivery. Before going into these topics, however, it is important to understand how genes and chromosomes affect development.[1]
Nature refers to the contribution of genetics to one’s development. The basic building block of the nature perspective is the gene. Genes are recipes for making proteins, while proteins influence the structure and functions of cells. Genes are located on the chromosomes and there are an estimated 20,500 genes for humans, according to the Human Genome Project.[2] See the box below for more details on the Human Genome Project.
The Human Genome Project
In 1990, the Human Genome Project (HGP), an international scientific endeavor, began the task of sequencing the 3 billion base pairs that make up the human genome. In April of 2003, more than two years ahead of schedule, scientists have given us the genetic blueprint for building a human. Since this time, using the information from the HGP, researchers have discovered the genes involved in over 1800 diseases. In 2005, the HGP amassed a large data base called HapMap that catalogs the genetic variations in 11 global populations. Data on genetic variation can improve our understanding of differential risk for disease and reactions to medical treatments, such as drugs. Pharmacogenomic researchers have already developed tests to determine whether a patient will respond favorably to certain drugs used in the treatment of breast cancer or HIV by using information from HapMap.
Future directions for the HGP include identifying the genetic markers for all 50 major forms of cancer (The Cancer Genome Atlas), continued use of the HapMap for creating more effective drugs for the treatment of disease, and examining the legal, social and ethical implications of genetic knowledge.
From the outset, the HGP made ethical issues one of their main concerns. Part of the HGP’s budget supports research and holds workshops that address these concerns. Who owns this information, and how the availability of genetic information may influence healthcare and its impact on individuals, their families, and the greater community are just some of the many questions being addressed.
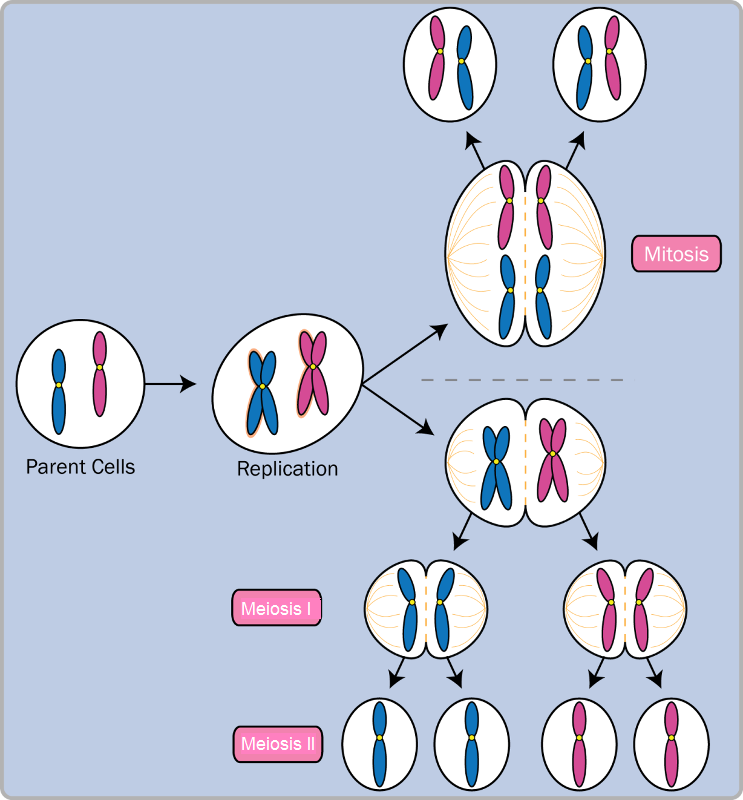
Normal human cells contain 46 chromosomes (or 23 pairs; one from each parent) in the nucleus of the cells. After conception, most cells of the body are created by a process called mitosis.
Mitosis is defined as the cell’s nucleus making an exact copy of all the chromosomes and splitting into two new cells. However, the cells used in sexual reproduction, called the gametes (sperm or ova), are formed in a process called meiosis. In meiosis the gamete’s chromosomes duplicate, and then divide twice resulting in four cells containing only half the genetic material of the original gamete. Thus, each sperm and egg possesses 23 chromosomes and combine to produce what is considered to be normative—a total of 46. See Figure 1 for details on both mitosis and meiosis. Given the amount of genes present and the unpredictability of the meiosis process, the likelihood of having offspring that are genetically identical (and not twins) is one in trillions.[3]
Of the 23 pairs of chromosomes created at conception, 22 pairs are similar in length. These are called autosomes. The remaining pair, or sex chromosomes, may differ in length. If a child receives the combination of XY the child will be genetically male. If the child receives the combination XX the child will be genetically female. Many genetic variations can occur within the sex chromosomes. For instance, people who have Turner syndrome typically have only one sex chromosome, an X, and people with Klinefelter syndrome have an extra X chromosome (XXY). See Table 2 below.
Genetic variations and inheritance
Genetic variation, the genetic differences between individuals, is what contributes to a species’ ability to adapt to its environment. In humans, genetic variation begins with an egg, several million sperm, and fertilization. The egg and the sperm each contain 23 chromosomes, which make up our genes. A single gene may have multiple possible variations or alleles (a specific version of a gene), resulting in a variety of combinations of inherited traits.
Genetic inheritance of traits for humans is based upon Gregor Mendel’s model of inheritance. For genes on an autosome (any chromosome other than a sex chromosome), the alleles and their associated traits are autosomal dominant or autosomal recessive. In this model, some genes are considered dominant because they will be expressed. Others, termed recessive, are only expressed in the absence of a dominant gene. Some characteristics that were once thought of as dominant-recessive, such as eye color, are now believed to be a result of the interaction between several genes.[4] Dominant traits include curly hair, facial dimples, normal vision, and dark hair. Recessive characteristics include red hair, pattern baldness, and nearsightedness.
Sickle cell anemia is an autosomal recessive disease; Huntington disease is an autosomal dominant disease. Other traits are a result of partial dominance or co-dominance in which both genes are influential. For example, if a person inherits both recessive genes for cystic fibrosis, the disease will occur. But if a person has only one recessive gene for the disease, the person would be a carrier of the disease.
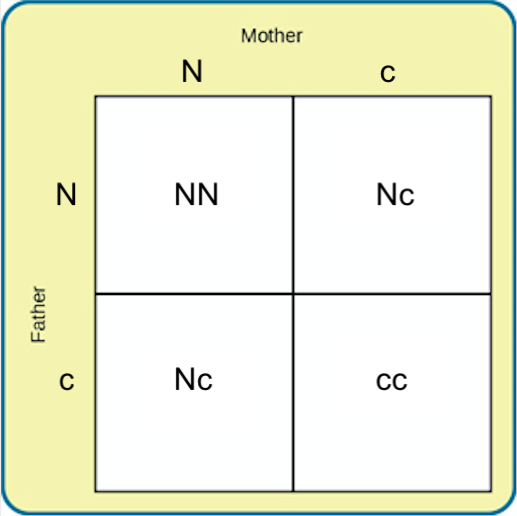
In this example, we will call the normal gene “N,” and the gene for cystic fibrosis “c.” The normal gene is dominant, which means that having the dominant allele either from one parent (Nc) or both parents (NN) will always result in the phenotype associated with the dominant allele. When someone has two copies of the same allele, they are said to be homozygous for that allele. When someone has a combination of alleles for a given gene, they are said to be heterozygous. For example, cystic fibrosis is a recessive disease which means that an individual will only have the disease if they are homozygous for that recessive allele (cc).
Imagine that a woman who is a carrier of the cystic fibrosis gene has a child with a man who also is a carrier of the same disease. What are the odds that their child would inherit the disease? Both the woman and the man are heterozygous for this gene (Nc). We can expect the offspring to have a 25% chance of having cystic fibrosis (cc), a 50% chance of being a carrier of the disease (Nc), and a 25% chance of receiving two normal copies of the gene (NN).
Gene mutations are one source of harmful genes. A mutation is a sudden, permanent change in a gene. While many mutations can be harmful or lethal, some mutations are beneficial by giving a person an advantage over those who do not have the mutation. Recall that the theory of evolution maintains that individuals best adapted to their particular environments are more likely to reproduce and pass on their genes to future generations. In order for this process to occur, there must be variability in genes (and resultant traits) that allow for variation in adaptability to the environment. If a population consisted of identical individuals, then any dramatic changes in the environment would affect everyone in the same way, and there would be no variation in selection. In contrast, diversity in genes and associated traits allows some individuals to perform slightly better than others when faced with environmental change. This creates a distinct advantage for individuals best suited for their environments in terms of successful reproduction and genetic transmission.
Genotypes and Phenotypes
The word genotype refers to the sum total of all the genes a person inherits. The word phenotype refers to the features that are actually expressed. Look in the mirror. What do you see, your genotype or your phenotype? What determines whether or not genes are expressed? Because genes are inherited in pairs on the chromosomes, we may receive either the same version of a gene from our mother and father, that is, be homozygous for that characteristic the gene influences. If we receive a different version of the gene from each parent, that is referred to as heterozygous. In the homozygous situation we will display that characteristic. It is in the heterozygous condition that it becomes clear that not all genes are created equal. Some genes are dominant, meaning they express themselves in the phenotype even when paired with a different version of the gene, while their silent partner is called recessive. Recessive genes express themselves only when paired with a similar version gene.
Geneticists refer to different versions of a gene as alleles. Some dominant traits include having facial dimples, curly hair, normal vision, and dark hair. Some recessive traits include red hair, being nearsighted, and straight hair.
Most characteristics are not the result of a single gene; they are polygenic, meaning they are the result of several genes. In addition, the dominant and recessive patterns described above are usually not that simple either. Sometimes the dominant gene does not completely suppress the recessive gene; this is called incomplete dominance. An example of this can be found in the recessive gene disorder sickle cell disease. The gene that produces healthy round-shaped red blood cells is dominant. The recessive gene causes an abnormality in the shape of red blood cells; they take on a sickle form, which can clog the veins and deprive vital organs of oxygen and increase the risk of stroke. To inherit the disorder a person must receive the recessive gene from both parents. Those who have inherited only one recessive-gene are called carriers and should be unaffected by this recessive trait. Yet, carriers of sickle cell have some red blood cells that take on the c-shaped sickle pattern. Under circumstances of oxygen deprivation, such as high altitudes or physical exertion, carriers for the sickle cell gene may experience some of the symptoms of sickle cell.[5]
Monozygotic and Dizygotic Twins
Many students are interested in twins. Monozygotic or identical twins occur when a fertilized egg splits apart in the first two weeks of development (Figure 3). The result is the creation of two separate, but genetically identical offspring. That is, they possess the same genotype and often the same phenotype.

About one-third of twins are monozygotic twins. Sometimes, however, two eggs or ova are released and fertilized by two separate sperm. The result is dizygotic or fraternal twins (Figure 4). These two individuals share the same amount of genetic material as would any two children from the same mother and father. In other words, they possess a different genotype and phenotype. Older mothers are more likely to have dizygotic twins than are younger mothers, and couples who use fertility drugs are also more likely to give birth to dizygotic twins. Consequently, there has been an increase in the number of fraternal twins recently.[6]

Genetic Disorders
Most known genetic disorders are dominant gene-linked; however, the vast majority of dominant gene linked disorders are not serious or debilitating. For example, the majority of those with Tourette’s Syndrome suffer only minor tics from time to time and can easily control their symptoms. Huntington’s Disease is a dominant gene linked disorder that affects the nervous system and is fatal, but does not appear until midlife. Recessive gene disorders, such as cystic fibrosis and sickle-cell anemia, are less common but may actually claim more lives because they are less likely to be detected, so people are unaware that they are carriers of the disease. Some genetic disorders are sex-linked; the defective gene is found on the X-chromosome. Males have only one X chromosome so are at greater risk for sex-linked disorders due to a recessive gene, such as hemophilia, color-blindness, and baldness. For females to be affected by the genetic defects, they need to inherit the recessive gene on both X-chromosomes, but if the defective gene is dominant, females can be equally at risk. Table 1 lists several genetic disorders.
| Recessive Disorders (Homozygous): The individual inherits a gene change from both parents. If the gene is inherited from just one parent, the person is a carrier and does not have the condition. | Cases per Birth |
| Sickle Cell Disease (SCD) is a condition in which the red blood cells in the body are shaped like a sickle (like the letter C) and affect the ability of the blood to transport oxygen. Carriers may experience some effects, but do not have the full condition. | 1 in 500 Black births
1 in 36,000 Hispanic births |
| Cystic Fibrosis (CF) is a condition that affects breathing and digestion due to thick mucus building up in the body, especially the lungs and digestive system. In
CF, the mucus is thicker than normal and sticky. |
1 in 3500 |
| Phenylketonuria (PKU) is a metabolic disorder in which the individual cannot metabolize phenylalanine, an amino acid. Left untreated intellectual deficits occur. PKU is easily detected and is treated with a special diet. | 1 in 10,000 |
| Tay Sachs Disease is caused by enzyme deficiency resulting in the accumulation of lipids in the nerve cells of the brain. This accumulation results in progressive damage to the cells and a decrease in cognitive and physical development. Death typically occurs by age five. | 1 in 4000
1in 30 American Jews is a carrier 1 in 20 French Canadians is a carrier |
| Albinism is when the individual lacks melanin and possesses little to no pigment in the skin, hair, and eyes. Vision problems can also occur. | Fewer than 20,000 US cases per year |
| Autosomal Dominant Disorders (Heterozygous): In order to have the disorder, the individual only needs to inherit the gene change from one parent. | Cases per Birth |
| Huntington’s Disease is a condition that affects the individual’s nervous system. Nerve cells become damaged, causing various parts of the brain to deteriorate. The disease affects movement, behavior and cognition. It is fatal, and occurs at midlife. | 1 in 10,000 |
| Tourette Syndrome is a tic disorder which results in uncontrollable motor and vocal tics as well as body jerking. | 1 in 250 |
| Achondroplasia is the most common form of disproportionate short stature. The individual has abnormal bone growth resulting in short stature, disproportionately short arms and legs, short fingers, a large head, and specific facial features. | 1 in 15,000-40,000 |
| Sex-Linked Disorders: When the X chromosome carries the mutated gene, the disorder is referred to as an X-linked disorder. Males are more affected than females because they possess only one X chromosome without an additional X chromosome to counter the harmful gene. | Cases per Birth |
| Fragile X Syndrome occurs when the body cannot make enough of a protein it needs for the brain to grow and problems with learning and behavior can occur. Fragile X syndrome is caused from an abnormality in the X chromosome, which then breaks. If a female has fragile X, her second X chromosome usually is healthy, but males with fragile X don’t have a second healthy X chromosome.
This is why symptoms of fragile X syndrome usually are more serious in males. |
1 in 4000 males
1 in 8000 females |
| Hemophilia occurs when there are problems in blood clotting causing both internal and external bleeding. | 1 in 10,000 males |
| Duchenne Muscular Dystrophy is a weakening of the muscles resulting in an inability to move, wasting away, and possible death. | 1 in 3500 males |
Chromosomal Variations
A chromosomal abnormality (or variation) occurs when a person inherits too many or too few chromosomes. The most common cause of chromosomal variations is the age of the mother. A 20-year-old woman has a 1 in 800 chance of having a child with a common chromosomal abnormality. A woman of 44, however, has a one in 16 chance. It is believed that the problem occurs when the ovum is ripening prior to ovulation each month. As the mother ages, the ovum is more likely to suffer abnormalities at this time.
Another common cause of chromosomal variations is that gametes do not divide evenly when they are forming. Therefore, some cells have more than 46 chromosomes. In fact, it is believed that close to half of all zygotes have an odd number of chromosomes. Most of these zygotes fail to develop and are spontaneously aborted by the body. If the abnormal number occurs on pair # 21 or # 23, however, the individual may have certain physical or other abnormalities. See Table 2 for additional information.
One of the most common chromosomal abnormalities is on pair # 21. Trisomy 21 occurs when there are three rather than two chromosomes on #21. A person with Down syndrome has distinct facial features, intellectual variations, and oftentimes heart and gastrointestinal disorders. Symptoms vary from person to person and can range from mild to severe. With early intervention, the life expectancy of persons with Down syndrome has increased in recent years. Keep in mind that there is as much variation in people with Down syndrome as in most populations and those differences need to be recognized and appreciated.
Watch the following video clip about Down syndrome from the National Down Syndrome Society:
You can view the transcript for “Down syndrome – Ability Awareness PSA Video” here (opens in new window).
| Autosomal Chromosome Disorders: The individual inherits too many or two few chromosomes. | Cases per Birth |
| Down syndrome/Trisomy 21 is caused by an extra chromosome 21 and includes a combination of birth defects. Affected individuals have some degree of intellectual variations, characteristic facial features, often heart defects, and other health problems. The severity varies greatly among affected individuals. | 1 in 691
1 in 300 births at age 35 |
| Trisomy 13 is caused by an extra chromosome 13. Affected individuals have multiple birth defects and generally die in the first weeks or months of life. | 1 in 7,906 |
| Trisomy 18 is caused by an extra chromosome 18 and the affected individual also has multiple birth defects within many areas of the body and typically results in early death. | 1 in 3,762 |
| Sex-Linked Chromosomal Disorders: The disorder occurs on chromosome pair #23 or the sex chromosomes. | Cases per Birth |
| Turner Syndrome is caused when all or part of one of the X chromosomes is lost before or soon after conception due to a random event. The resulting zygote has an XO composition. Turner Syndrome typically affects cognitive functioning and sexual maturation in girls. Infertility and a short stature may be noted. | 1 in 2500 females |
| Klinefelter Syndrome is caused when an extra X chromosome is present in the cells of a male due to a random event. The Y chromosome stimulates the growth of male genitalia, but the additional X chromosome inhibits this development. The male may have some breast development, infertility, and low levels of testosterone. | 1 in 700 males |
Genetic Counseling
Genetic counseling refers to a service that assists individuals identify, test for, and explain potential genetic conditions that could adversely affect themselves or their offspring.[7] The more common reasons for genetic counseling include:
- Family history of a genetic condition.
- Membership in a certain ethnic group with a higher risk of a genetic condition.
- Information regarding the results of genetic testing, including blood tests, amniocentesis, or ultrasounds.
- Learning about the chances of having a baby with a genetic condition if the mother is older, has had several miscarriages, has offspring with birth defects, experiences infertility, or has a medical condition.
Behavioral Genetics
Behavioral Genetics is the scientific study of the interplay between the genetic and environmental contributions to behavior. Often referred to as the nature/nurture debate, Gottlieb suggests an analytic framework for this debate that recognizes the interplay between the environment, behavior, and genetic expression.[8] This bidirectional interplay suggests that the environment can affect the expression of genes just as genetic predispositions can impact a person’s potentials. Additionally, environmental circumstances can trigger symptoms of a genetic disorder. For example, a person who has sickle cell anemia, a recessive gene linked disorder, can experience a sickle cell crisis under conditions of oxygen deprivation. Someone predisposed genetically for type-two diabetes can trigger the disease through poor diet and little exercise.
Research has shown how the environment and genotype interact in several ways. Genotype- environment correlations refer to the processes by which genetic factors contribute to variations in the environment.[9] There are three types of genotype-environment correlations:
Passive genotype-environment correlation occurs when children passively inherit the genes and the environments their family provides. Certain behavioral characteristics, such as being athletically inclined, may run in families. The children have inherited both the genes that would enable success at these activities, and given the environmental encouragement to engage in these actions.
Evocative genotype-environment correlation refers to how the social environment reacts to individuals based on their inherited characteristics. For example, whether one has a more outgoing or shy temperament will affect how they are treated by others.
Active genotype-environment correlation occurs when individuals seek out environments that support their genetic tendencies. This is also referred to as niche picking. For example, children who are musically inclined seek out music instruction and opportunities that facilitate their natural musical ability.
Conversely, genotype-environment interactions involve genetic susceptibility to the environment. Adoption studies provide evidence for genotype-environment interactions. For example, the Early Growth and Development Study followed 360 adopted children and their adopted and biological parents in a longitudinal study.[10] Results revealed that children whose biological parents exhibited psychopathology, exhibited significantly fewer behavior problems when their adoptive parents used more structured parenting than unstructured. Additionally, elevated psychopathology in adoptive parents increased the risk for the children’s development of behavior problems, but only when the biological parents’ psychopathology was high. Consequently, the results demonstrate how environmental effects on behavior differ based on the genotype, especially stressful environments on genetically at-risk children.
Lastly, epigenetics studies modifications in DNA that affect gene expression and are passed on when the cells divide. Environmental factors, such as nutrition, stress, and teratogens are thought to change gene expression by switching genes on and off. These gene changes can then be inherited by daughter cells. This would explain why monozygotic or identical twins may increasingly differ in gene expression with age. For example, Fraga et al. (2005) found that when examining differences in DNA, a group of monozygotic twins were indistinguishable during the early years.[11] However, when the twins were older there were significant discrepancies in their gene expression, most likely due to different experiences. These differences included susceptibilities to disease and a range of personal characteristics.
- This chapter was adapted from select chapters in Lumen Learning's Lifespan Development, authored by Martha Lally and Suzanne Valentine-French available under a Creative Commons Attribution-NonCommercial-ShareAlike license, and Waymaker Lifespan Development by Lumen Learning and available under a Creative Commons Attribution license. Some selections from Lumen Learning were adapted from previously shared content from Laura Overstreet's Lifespan Psychology and Wikipedia. ↵
- National Institute of Health (2015). An overview of the human genome project. http://www.genome.gov/12011238 ↵
- Gould, J. L., & Keeton, W. T. (1997). Biological science (6th ed.). New York: Norton. ↵
- McKusick, V. A. (1998). Mendelian inheritance in man: A catalog of human genes and genetic disorders. Baltimore, MD: Johns Hopkins University Press. ↵
- Berk, L. (2004). Development through the life span (3rd ed.). Boston: Allyn and Bacon. ↵
- Bortolus, R., Parazzini, F., Chatenoud, L., Benzi, G., Bianchi, M. M., & Marini, A. (1999). The epidemiology of multiple births. Human Reproduction Update, 5, 179-187. ↵
- Centers for Disease Control and Prevention. (2015) Genetic Counseling. Retrieved from http://www.cdc.gov/ncbddd/genetics/genetic_counseling.html ↵
- Gottlieb, G. (2002). Individual development and evolution: The genesis of novel behavior. New York: Oxford University Press. ↵
- Plomin, R., DeFries, J. C., Knopik, V. S., & Niederhiser, J. M. (2013). Behavioral Genetics (6th edition). NY: Worth Publishers. ↵
- Leve, L. D., Neiderhiser, J. M., Scaramella, L. V., & Reiss, D. (2010). The early growth and development study: using the prospective adoption design to examine genotype-environment interplay. 2008. Behavior Genetics, 40(3), 306–314. https://doi.org/10.1007/s10519-010-9353-1 ↵
- Fraga, M. F., Ballestar, E., Paz, M. F., Ropero, S., Setien, F., Ballestar, M. L., Heine-Suñer, D., Cigudosa, J. C., Urioste, M., Benitez, J., Boix-Chornet, M., Sanchez-Aguilera, A., Ling, C., Carlsson, E., Poulsen, P., Vaag, A., Stephan, Z., Spector, T. D., Wu, Y.-Z., … Esteller, M. (2005). Epigenetic differences arise during the lifetime of monozygotic twins. Proceedings of the National Academy of Sciences of the United States of America, 102(30), 10604–10609. https://doi.org/10.1073/pnas.0500398102 ↵

{kind=link}